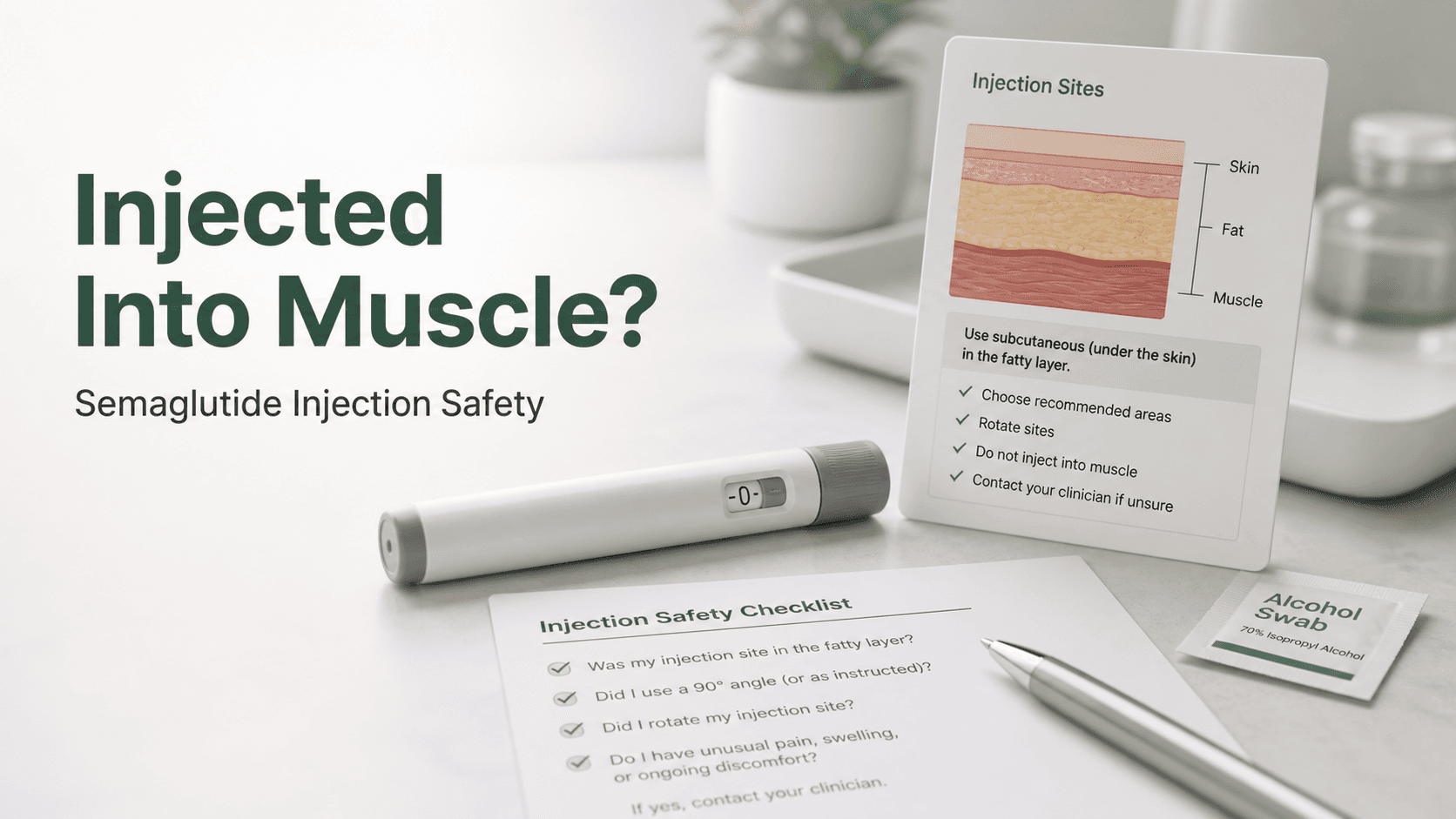
Semaglutide injections are intended to go under the skin, not into muscle.
Short answer: if you think semaglutide was injected into muscle, do not repeat the dose. Monitor for unusual side effects, low blood sugar symptoms if diabetic or on glucose-lowering medications, worsening pain, swelling, redness, or infection signs. Contact the prescriber or pharmacist for guidance.
What to Watch
| Symptom | Why it matters |
|---|---|
| Increasing pain or swelling | Injection injury or irritation |
| Redness, warmth, pus, fever | Infection concern |
| More nausea than usual | Possible altered absorption or dose sensitivity |
| Low blood sugar symptoms | More important with diabetes medications |
Preventing Repeat Errors
Use the product's approved injection sites, confirm needle length and device type, avoid tense muscle, and ask for injection training if you are unsure.
Internal Reading Path
The GLP-1 Nutrition Filter
For accidentally injected semaglutide into muscle, the goal is not to create a stricter diet. The goal is to make a smaller appetite nutritionally useful. A good GLP-1 plan protects protein, fluids, fiber, micronutrients, and muscle while reducing the foods or habits that trigger side effects.
A helpful filter is to ask four questions before a meal: Where is the protein? Is the portion small enough to tolerate? Is there a fiber source that will not worsen bloating? Have fluids been steady today? If the answer is no to several of those questions, the meal may be filling but not supportive.
| Priority | Practical examples |
|---|---|
| Protein | Greek yogurt, eggs, fish, poultry, tofu, cottage cheese, beans, protein shake |
| Gentle carbs | Rice, oats, potatoes, toast, fruit, soup noodles |
| Fiber | Berries, oats, cooked vegetables, beans, chia, ground flax |
| Fluids | Water, low-sugar electrolytes, broth, non-carbonated drinks |
| Tolerance | Smaller meals, slower eating, lower-fat choices during escalation |
Small Appetite Meal Strategy
When appetite is very low, trying to eat a normal-sized meal can worsen nausea or reflux. A smaller meal schedule often works better. Think in protein anchors rather than large plates: yogurt plus fruit, eggs plus toast, soup with shredded chicken, tofu with rice, cottage cheese with berries, or a smoothie with protein and a gentle carbohydrate.
If intake is too low for several days, symptoms like fatigue, dizziness, constipation, headache, poor workouts, and hair shedding risk can become more likely. That is a reason to discuss the dose and nutrition plan, not a sign that the medication is working perfectly.
Adjustments by Side Effect
| If this is happening | Try discussing or testing |
|---|---|
| Nausea | Smaller meals, lower fat, slower eating, bland protein |
| Constipation | More fluids, gradual fiber, regular meals, movement |
| Diarrhea | Lower-fat reset, electrolytes, review sugar alcohols |
| Reflux | Earlier dinner, less carbonation, stay upright after meals |
| Fatigue | Protein, hydration, electrolytes, sleep, dose review |
Questions to Bring to the Prescriber or Pharmacist
- Does my current dose and timing match the official label or my prescription?
- Are my symptoms or concerns expected at this stage, or do they suggest changing the plan?
- Should I delay escalation, restart lower, hold steady, or be evaluated before continuing?
- Are any of my other medications increasing risk, especially insulin, sulfonylureas, blood pressure medication, diuretics, or drugs affected by delayed gastric emptying?
- What exact symptoms should make me call urgently or seek same-day care?
- If cost or supply interrupts therapy, what is the safest backup plan?
Bottom Line for Accidentally Injected Semaglutide Into Muscle: What to Do Next
The practical answer is rarely just one number, food list, or yes-or-no rule. For accidentally injected semaglutide into muscle, the safest approach is to combine the direct answer with the variables that change it: product type, dose, timing, side effects, storage history, other medications, and the person's medical context. When those variables are unclear, the best next step is to ask the prescriber or pharmacist before acting.
Additional Scenarios Readers Commonly Compare
| Scenario | How to think about it |
|---|---|
| Symptoms started after a dose increase | Treat escalation as a likely contributor and ask whether to hold the dose longer |
| The plan changed because of supply | Confirm whether a restart or lower dose is safer after the gap |
| Advice online conflicts with the label | Use the label, pharmacy, and prescriber as the authority |
| The medication is compounded | Verify concentration, BUD, storage, sterility, and dose instructions directly with the pharmacy |
| The goal is maintenance | Prioritize sustainable intake, resistance training, monitoring, and follow-up |
More FAQ
Why do different websites give different answers?
Most differences come from assuming different products, concentrations, patient goals, dose histories, or risk tolerance. A chart or tip can be mathematically correct but still wrong for a specific prescription.
What information should I keep in my notes?
Keep the medication name, dose, date taken, pharmacy label, concentration if vial-based, side effects, food and fluid changes, weight trend, and any clinician instructions. This makes follow-up safer and more specific.
When is it better not to troubleshoot at home?
Do not troubleshoot at home when symptoms are severe, rapidly worsening, involve chest pain or fainting, include repeated vomiting or dehydration, suggest allergic reaction, or involve a possible dosing or storage error.
Quick Self-Check Before Acting
Before making a decision based on accidentally injected semaglutide into muscle, pause long enough to confirm the basics: exact medication, dose, date of last dose, product form, storage history if relevant, current symptoms, and any other medications that could change risk. Most GLP-1 mistakes happen when one of those details is assumed instead of verified.
If the question involves dosing, switching, storage, severe symptoms, pregnancy planning, surgery, diabetes medication, or a compounded vial, treat the article as preparation for a clinician or pharmacist conversation. The safest next step is often not to act faster. It is to bring better information to the person who can make the decision with you.
| Detail to confirm | Why it matters |
|---|---|
| Medication and form | Pens, tablets, branded vials, and compounded vials have different rules |
| Current dose | Dose history changes tolerance and restart decisions |
| Timing | Missed doses, gaps, and dose increases change the plan |
| Symptoms | Severity decides whether this is routine or urgent |
| Storage or expiration | Product reliability depends on label and pharmacy rules |
| Other medications | Insulin, sulfonylureas, blood pressure drugs, and diuretics can change risk |
Final Reminder
This is exactly the kind of GLP-1 question where the safest next step depends on details that may not be obvious from memory. Keep the product box, pharmacy label, dose history, and symptom notes available. If the situation involves uncertainty, do not solve it by repeating a dose, guessing a conversion, or relying on a social-media answer. Use the information here to ask a more precise question and get a safer answer.
Summary
Do not re-dose after a suspected intramuscular semaglutide injection. Monitor, document what happened, and ask the care team how to proceed.
References
- U.S. Food and Drug Administration. WEGOVY (semaglutide) injection — Prescribing Information. (Semaglutide is for subcutaneous injection in the abdomen, thigh, or upper arm.)
- Collins L, Costello RA. Glucagon-Like Peptide-1 Receptor Agonists. StatPearls, NCBI Bookshelf. (Hypoglycemia risk with insulin/sulfonylureas; GLP-1 administration and effects.)