


GLP-1 gets the headlines, but it is the addition of GIP — a different incretin hormone the body releases after eating — that made tirzepatide outperform every GLP-1-only drug on the market. The surprise from the molecular pharmacology data: tirzepatide actually binds the GLP-1 receptor about 5× weaker than native GLP-1 and 13× weaker than semaglutide. Its weight-loss advantage comes from full-strength GIP receptor activation, plus a clever "biased agonism" signaling profile that boosts insulin output without triggering the usual GLP-1 nausea ceiling.
GLP-1 is one of several gut hormones; see how it compares in GLP-1 vs GLP-2.
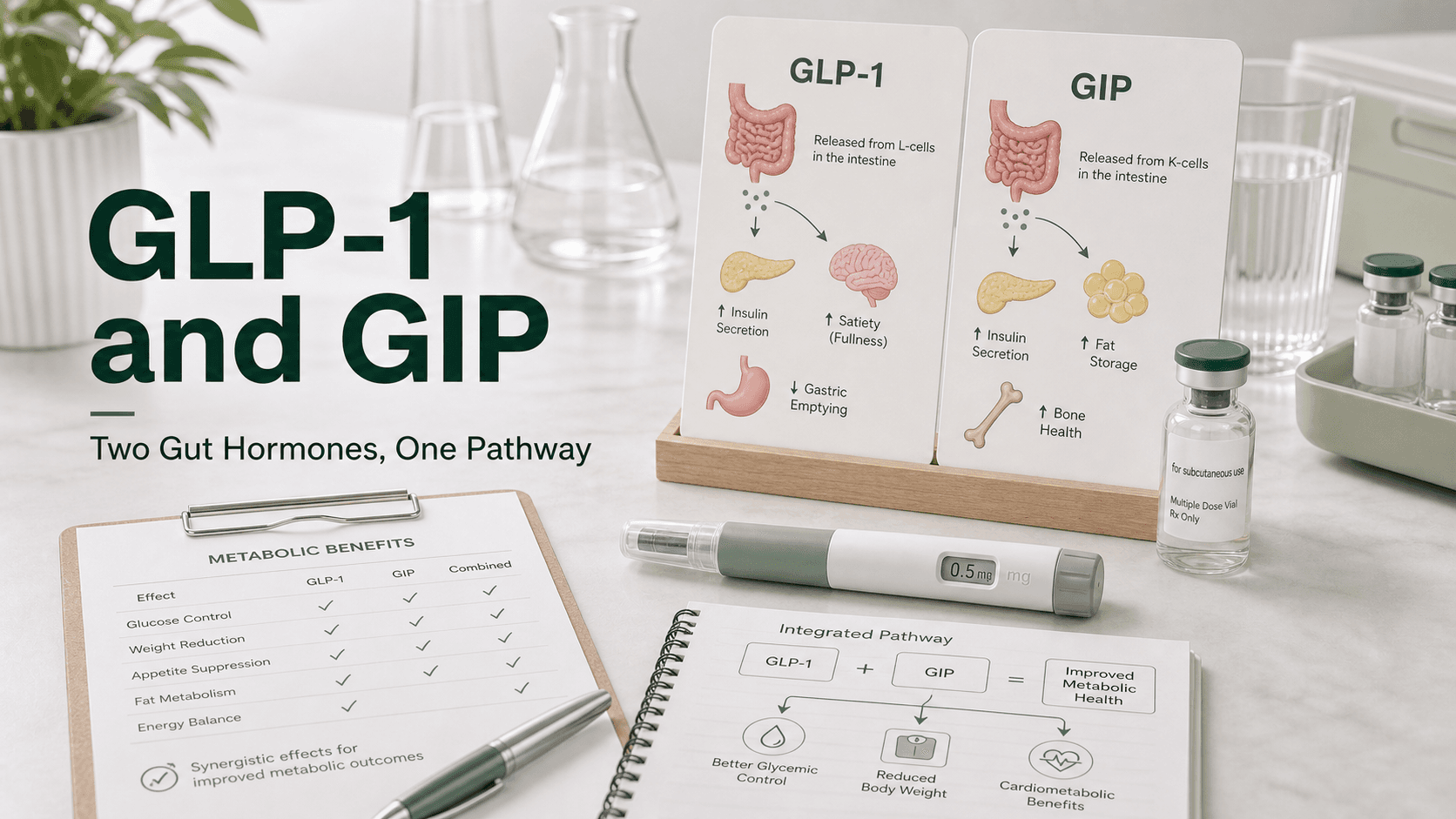
Direct answer: GLP-1 and GIP are the two incretin hormones released by gut L-cells and K-cells after a meal. Both trigger insulin release, but their downstream effects differ. GLP-1 strongly slows gastric emptying, suppresses appetite, and quiets food noise. GIP improves insulin sensitivity, modifies fat tissue energy storage, and appears to buffer the nausea caused by GLP-1. Tirzepatide (Mounjaro, Zepbound) is the first FDA-approved drug to activate both — its dual mechanism explains why it produces ~21% mean weight loss in obesity trials vs ~15% for semaglutide. Retatrutide adds a third receptor (glucagon) for even higher weight loss.
The Two Incretins, Side By Side
| GLP-1 | GIP | |
|---|---|---|
| Full name | Glucagon-like peptide-1 | Glucose-dependent insulinotropic polypeptide |
| Released from | L-cells (ileum, colon) | K-cells (duodenum, jejunum) |
| Half-life (native) | ~2 minutes | ~7 minutes |
| Receptor | GLP-1R | GIPR |
| Insulin release | Yes, glucose-dependent | Yes, glucose-dependent |
| Slows gastric emptying | Strongly | Modestly |
| Reduces appetite | Strongly (via brain receptors) | Indirectly |
| Effect on glucagon | Suppresses | Increases in some contexts |
| Effect on fat tissue | Modest | Direct — improves insulin sensitivity |
| Effect on bone | Minimal | Promotes bone formation |
Both hormones are released within minutes of food hitting the small intestine. Together they produce the incretin response — the reason oral glucose triggers a much bigger insulin spike than the same amount of glucose given by IV.
What GLP-1 Does in Detail
GLP-1 receptors are present in the pancreas, stomach, gut, and brain. Activating them:
- Triggers glucose-dependent insulin release (only when blood sugar is high — minimal hypoglycemia risk alone)
- Slows gastric emptying so meals enter the bloodstream gradually
- Reduces appetite through receptors in the hypothalamus and brainstem
- Quiets "food noise" — intrusive thoughts about food
- Suppresses glucagon, preventing liver glucose dumping
- May protect heart and kidney tissue via anti-inflammatory effects (SELECT and FLOW outcome data)
This is what semaglutide, liraglutide, dulaglutide, and exenatide all do — pure GLP-1 receptor agonism.
What GIP Adds
GIP was discovered before GLP-1 and was originally dismissed for diabetes because diabetics have a blunted GIP response. Tirzepatide's data forced a rethink.
GIP receptor activation:
- Triggers insulin release, especially after large meals
- Improves insulin sensitivity in muscle and fat tissue
- Buffers fat storage — appears to help fat tissue handle energy more efficiently
- Appears to soften nausea triggered by GLP-1, allowing higher tolerated doses
- Has less effect on stomach emptying and appetite than GLP-1 alone
That last point is critical: pure GLP-1 drugs are limited by how much GI side effects patients can tolerate during titration. Adding GIP appears to soften nausea at any given level of weight loss.
The Imbalanced Agonism Behind Tirzepatide
This is where the pharmacology gets interesting. Tirzepatide is a single 39-amino-acid peptide engineered to bind both receptors, but the binding is deliberately imbalanced:
| Property | Tirzepatide at GIPR | Tirzepatide at GLP-1R |
|---|---|---|
| Binding affinity (vs native hormone) | Equipotent with native GIP | ~5× weaker than native GLP-1 |
| Functional potency (cAMP) | Equivalent to native GIP | ~20× weaker than native GLP-1 |
| Comparison to semaglutide | N/A | ~13× weaker at GLP-1R |
| β-arrestin recruitment | Full agonist | Partial (<10% Emax — only 40% of GLP-1's max effect) |
| Receptor internalization | Equivalent to GIP (~35%) | Minimal (40% of what GLP-1 causes) |
The headline: tirzepatide is a weaker GLP-1 agonist than semaglutide. Its advantage is GIP — and a clever "biased" signaling profile at GLP-1R that emphasizes cAMP over β-arrestin.
Why the β-Arrestin Bias Matters
β-arrestin normally "restrains" GLP-1R signaling, dampening insulin release. Tirzepatide's reduced β-arrestin recruitment means it bypasses this restraining mechanism — actually enhancing insulin output per unit of GLP-1R activation. Knockout mouse experiments confirmed this: removing β-arrestin1 boosted insulin response to GLP-1 but not to tirzepatide, because tirzepatide already operates around the brake.
Albumin Binding and Once-Weekly Dosing
Tirzepatide contains a C20 unsaturated di-acid acyl chain that binds human serum albumin with a Kd of 1.86 μM. This albumin binding:
- Extends the half-life to ~5 days
- Enables once-weekly subcutaneous dosing
- Right-shifts in-vitro potency 26× at GIPR and 81× at GLP-1R (the body is "carrying" much of the drug bound to albumin)
Predicted Receptor Occupancy at Clinical Doses
This is the cleanest way to see why tirzepatide's clinical results favor GIP:
| Dose | GIPR occupancy | GLP-1R occupancy |
|---|---|---|
| Tirzepatide 5 mg/week | ~18% | ~3% |
| Tirzepatide 15 mg/week | ~52% | ~10% |
| Semaglutide 1 mg/week | — | ~6% |
At 15 mg tirzepatide, GIP receptor engagement is 5× GLP-1 receptor engagement. The drug is, functionally, much more of a GIP agonist than a GLP-1 agonist in vivo.
Why Dual Agonists Beat Single Agonists Clinically
Across trials, the pattern is consistent:
| Drug | Receptors hit | Avg weight loss at top dose, ~72 weeks |
|---|---|---|
| Liraglutide | GLP-1 | ~6% (SCALE) |
| Semaglutide 2.4 mg | GLP-1 | ~15% (STEP) |
| Tirzepatide 15 mg | GLP-1 + GIP | ~21% (SURMOUNT-1) |
| Retatrutide 12 mg | GLP-1 + GIP + glucagon | ~24% (Phase 2) |
The SURMOUNT-1 trial (2,539 non-diabetic obese participants, 72 weeks):
- 5 mg tirzepatide: 15.0% weight loss
- 10 mg tirzepatide: 19.5% weight loss
- 15 mg tirzepatide: 20.9% weight loss
- Placebo: 3.1% weight loss
- 50–57% of patients on 10–15 mg achieved ≥20% weight loss
What GIP Does To Insulin Sensitivity (Beyond Weight Loss)
A critical finding from beta-cell function studies: weight loss explained only 13% to 21% of the improvement in insulin resistance seen with tirzepatide at 10 mg and 15 mg. The remaining improvement is directly attributable to the dual receptor activation.
Specific markers improved at high doses:
- HOMA2-B (beta-cell function) significantly increased
- HOMA2-IR (insulin resistance) significantly decreased (P = 0.004 at 10 mg)
- Adiponectin levels increased 12–26%
- IGFBP-2 levels increased 38–89%
- Proinsulin/insulin ratios decreased — less beta-cell stress
This is metabolic improvement that semaglutide does not produce to the same degree.
A1C Reductions in Diabetes Trials
In the SURPASS program for type 2 diabetes:
| Trial | Comparison | A1C reduction with tirzepatide |
|---|---|---|
| SURPASS-1 | Placebo | 1.87–2.07 percentage points |
| SURPASS-2 | Semaglutide 1 mg | Superior to semaglutide |
| SURPASS-3 | Insulin degludec | 1.93–2.37 percentage points |
| SURPASS-4 | Insulin glargine | 2.24–2.58 percentage points |
Body weight reductions paralleled: SURPASS-2 showed tirzepatide produced 1.9–5.5 kg more weight loss than semaglutide.
Side Effects of Dual Agonism
GI side effects dominate, similar to GLP-1-only drugs:
| Side effect | Rate on tirzepatide |
|---|---|
| Nausea | 12–18% |
| Diarrhea | 12–17% |
| Vomiting | 5–9% |
| Discontinuation due to AEs | 3.0–6.6% |
Hypoglycemia remains low unless combined with insulin or sulfonylureas. Cardiovascular safety data so far show no excess risk (MACE-4 HR ~0.80 in early meta-analysis; SURPASS-CVOT is the definitive outcome trial).
The Glucagon Question (Retatrutide)
Retatrutide is the next step up: a triple agonist that hits GLP-1, GIP, and glucagon receptors. Glucagon normally raises blood sugar, so adding it to a weight-loss drug sounds counterintuitive. The mechanism:
- Glucagon increases energy expenditure — basal metabolic rate goes up
- The GLP-1 component suppresses the blood-sugar rise that glucagon would normally cause
- The GIP component buffers tolerability at high doses
In Phase 2 trials, retatrutide 12 mg produced ~24% weight loss at 48 weeks — the highest seen for any anti-obesity drug to date. It is not FDA approved yet; Phase 3 readouts are ongoing in 2026.
What GIP Alone Would Do
There are no FDA-approved pure GIP agonists. Animal data is interesting:
- In healthy mice, pure GIP boosts insulin response with little weight loss
- In obese mice, GIP analogues actually reduce body weight — opposite to early expectations
- The leading hypothesis: GIP amplifies GLP-1's effects on brain energy regulation
This explains why tirzepatide outperforms semaglutide despite weaker GLP-1 binding.
What People Get Wrong About GLP-1 and GIP
- "GIP is just another name for GLP-1." Completely different peptides, released from different cells, with different (overlapping) effects.
- "Tirzepatide is a stronger GLP-1." Its GLP-1R activity is actually weaker than semaglutide. The advantage comes from GIP plus biased β-arrestin signaling.
- "Adding glucagon will spike blood sugar." In retatrutide, the GLP-1 effect dominates blood sugar, while glucagon contributes calorie burn.
- "Only GLP-1 matters for weight loss." SURMOUNT-1 data argues otherwise — adding GIP added ~6 percentage points of weight loss.
Frequently Asked Questions
What is the difference between GLP-1 and GIP? Both are gut incretin hormones that trigger insulin release after meals. GLP-1 also strongly slows stomach emptying and reduces appetite. GIP works more on fat tissue, insulin sensitivity, and tolerability.
Why is tirzepatide called a dual agonist? Because the single molecule activates both the GLP-1 receptor and the GIP receptor.
Is Mounjaro a GLP-1 or GIP drug? Both. Mounjaro and Zepbound (same molecule, different indications) are dual GLP-1 + GIP receptor agonists.
Does GIP cause nausea like GLP-1? Less so. Adding GIP appears to soften the nausea that limits GLP-1-only drugs at high doses.
Is tirzepatide a stronger GLP-1 than semaglutide? No — it actually binds the GLP-1 receptor about 13× weaker than semaglutide. The advantage comes from the added GIP activity and the biased β-arrestin signaling profile.
Is GIP available as a standalone drug? No. There are no FDA-approved pure GIP agonists. GIP is currently only available as part of tirzepatide.
Last reviewed: May 13, 2026




