


Dermatologist Dr. Paul Jarrod Frank coined the term "Ozempic face" in 2022 to describe the hollow cheeks, sunken temples, and loose skin around the jawline that show up after months on a GLP-1. For a long time the assumption was: it is just rapid weight loss, same as bariatric surgery face. New research suggests something more specific — GLP-1 receptors on adipose-derived stem cells directly affect collagen synthesis, oxidative stress, and dermal fat, which may explain why the face seems to age faster than the rest of the body on these drugs.
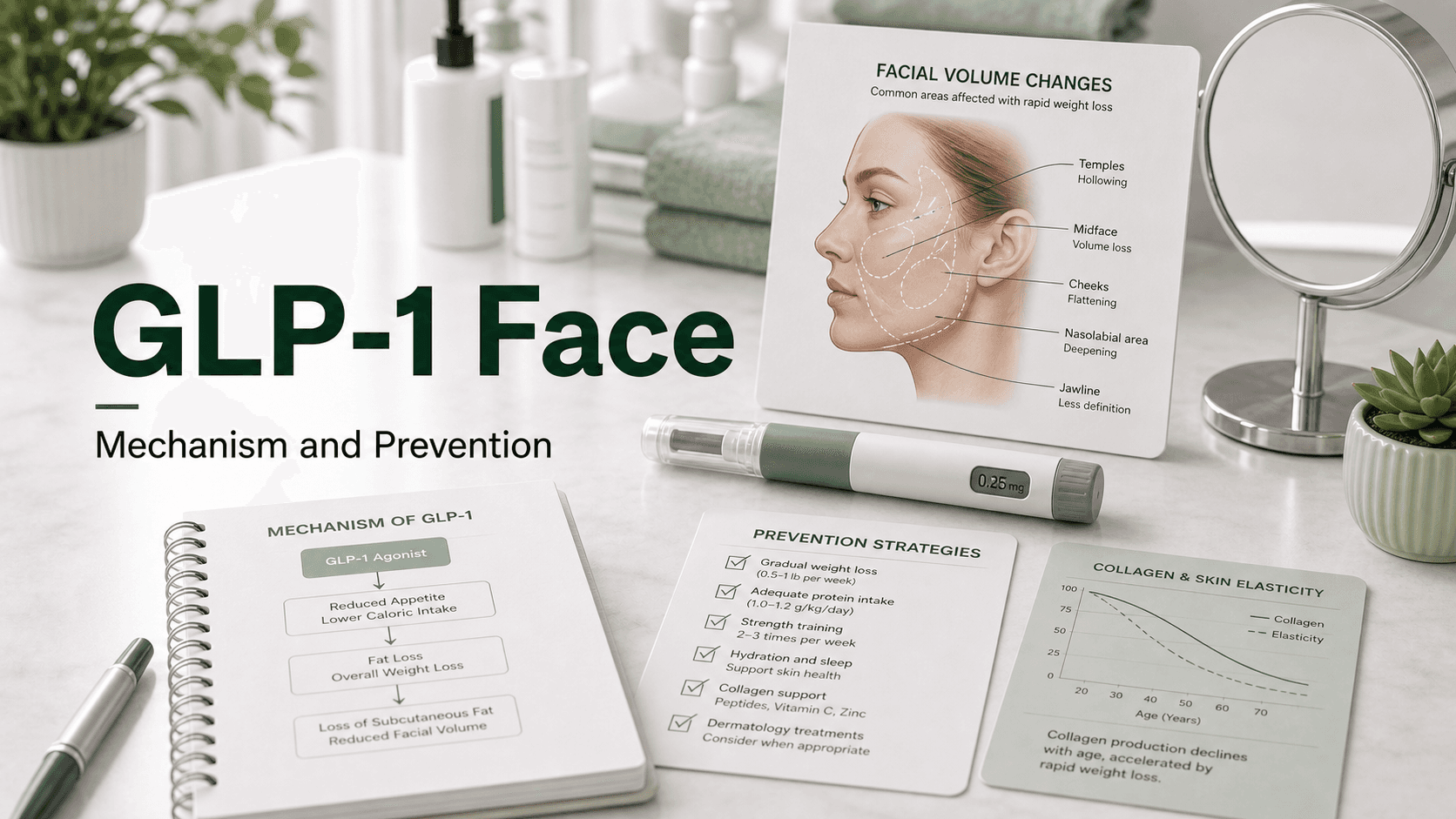
Direct answer: "Ozempic face" or "GLP-1 face" describes the gaunt, sunken, and aged appearance that can follow rapid weight loss on a GLP-1. The main driver is loss of subcutaneous and dermal white adipose tissue (DWAT) combined with reduced collagen and elastin. New mechanistic data shows GLP-1 receptors on adipose-derived stem cells (ADSCs) reduce their cytokine output, triggering oxidative damage to fibroblasts and matrix metalloproteinase-1 activity that breaks down collagen. It typically becomes visible after losing 15–20 lb or 10–20% of body weight over 2–6 months. Slower titration, adequate protein, strength training, sleep, and sun protection reduce severity. Once it appears: dermal fillers, biostimulatory injectables (Sculptra), microneedling/RF (Sofwave), fat grafting, or surgical facelift.
What Is Actually Happening
The mechanism is more layered than "you lost weight too fast." Three things are happening at once:
1. Loss of Subcutaneous Facial Fat
Rapid weight loss shrinks the fat that cushions the cheeks, temples, and under-eyes. The cheeks hollow, temples sink, jawline shows more bone. Mechanical, predictable.
2. Loss of Dermal White Adipose Tissue (DWAT)
Distinct from the subcutaneous fat layer, DWAT is the thin layer of fat within the skin itself. GLP-1 drugs appear to deplete it disproportionately. Less DWAT = less skin volume and faster wrinkling.
3. Direct GLP-1 Effects on Skin Cells
This is the new piece. GLP-1 receptors exist on adipose-derived stem cells (ADSCs) in the skin. Activation:
- Reduces ADSC production of protective cytokines, triggering oxidative damage to fibroblasts (the cells that make collagen and elastin)
- Decreases estrogen production from ADSCs, which normally stimulates fibroblast collagen synthesis
- Increases matrix metalloproteinase-1 activity, which breaks down existing collagen
- Increases reactive oxygen species (ROS) production in ADSCs, damaging cell membranes and signaling
The combined effect is faster collagen and elastin loss than would happen from weight loss alone — which is part of why "Ozempic face" looks different from "post-diet" face.
Who Gets It Worst
| Risk factor | Why it matters |
|---|---|
| Age 40+ | Lower baseline collagen, slower remodeling |
| Faster weight loss rate | Less time for skin to adapt |
| Larger total weight loss | More volume change |
| Female sex | Slightly thinner skin, less retentive sub-Q fat |
| Sun damage / smoking history | Reduced elastin reserve |
| Lower starting body fat | Less to lose before face shows it |
| Low protein intake | Collagen synthesis impaired |
| Sleep deprivation | Skin remodeling occurs largely in deep sleep |
| Higher GLP-1 dose | Faster weight loss, more direct cell effect |
When It Appears
Most people start seeing changes around the 15–20 lb mark, which on a GLP-1 typically lands at month 3–4. The change accelerates between months 4 and 9, when weight loss is at peak rate.
After weight stabilizes (month 12+), the face often "settles" over the following 6–12 months as collagen partially rebuilds.
Per Cleveland Clinic endocrinologist Dr. Vinni Makin:
"The faster your weight loss, the more likely that your face will show signs of the weight loss."
How To Reduce It Before It Starts
1. Slow Down the Rate of Loss
The single biggest variable. Losing 1–1.5 lb/week is much easier on the face than 3 lb/week.
- Don't push past the lowest tolerated dose to chase faster results
- Skip a titration step if losing too fast
- Stay at a maintenance dose once you reach your target weight
2. Eat Enough Protein
Adequate protein supports skin and lean-mass preservation:
- Target 1.2–1.6 g/kg of body weight per day (about 0.55–0.73 g/lb)
- For a 180-lb person: ~100–130 g protein/day
- Prioritize meals over shakes when possible
3. Strength Train
- Preserves lean body mass, so weight loss is mostly fat
- Improves circulation and nighttime growth-hormone pulses that drive skin remodeling
- 2–3× per week minimum
4. Sleep 7–9 Hours
Skin remodeling occurs primarily during slow-wave sleep. Cutting sleep cuts collagen turnover. One of the simplest, most-overlooked steps.
5. Stay Hydrated
GLP-1s blunt thirst signals. Dehydration exaggerates facial hollowness. Aim for ~half your body weight (in lb) in ounces of fluid daily.
6. Sun Protection
Loss of skin support is permanent if structural proteins are already sun-damaged. Daily SPF 30+ protects what's left.
7. Don't Overshoot Your Target
Set a stopping weight and back off the dose when you reach it. The medication keeps suppressing appetite past your goal weight if you let it.
What Helps When It Already Happened
Cosmetic dermatology and plastic surgery options, in order of invasiveness:
| Treatment | What it does | Typical duration |
|---|---|---|
| Topical retinoids + peptides | Modest collagen remodeling | Months of daily use |
| Microneedling + radiofrequency (e.g., Morpheus8) | Stimulates collagen | 6–12 months per series |
| Sofwave (ultrasound) | Collagen stimulation | 6–12 months |
| Hyaluronic acid fillers (Juvéderm, Restylane) | Replaces lost volume | 9–18 months |
| Sculptra (poly-L-lactic acid) | Triggers collagen growth | 2+ years |
| Platelet-rich plasma (PRP) | Growth factors for skin | Adjunct to other procedures |
| Botox | Wrinkles, not volume | 3–4 months |
| Fat grafting | Transplants patient's own fat | Long-lasting (some resorption) |
| Threads (PDO/PLLA) | Mechanical lift + collagen | 6–12 months |
| Facelift / neck lift | Surgical excess-skin removal | Years to decades |
| Blepharoplasty | Excess eyelid skin | Long-term |
| Lip lift | Restores upper lip shape | Long-term |
Most patients start with sub-surgical options (fillers, microneedling) and reserve surgical lifts for severe laxity after weight has stabilized for 6–12 months.
Doesn't Some of It Come Back?
Yes, partially. Once weight is stable:
- Subcutaneous fat can partially return over 6–12 months as the body recalibrates
- Skin remodeling continues for 12–24 months
- Late-onset improvement is common, especially in younger patients with better skin reserve
This is part of why most cosmetic surgeons recommend waiting 6–12 months after weight stabilizes before pursuing a definitive procedure.
What People Get Wrong
- "GLP-1 melts facial fat selectively." Partly true — direct GLP-1 effects on dermal adipose tissue and stem cells amplify the rapid weight-loss effect.
- "Only Ozempic does this." All rapid weight loss does, but GLP-1s appear to add a direct cellular component.
- "Eating more will fix it." Eating more raises overall fat percentage, but the face isn't the first place fat returns. Better to slow the loss in the first place.
- "I should stop the medication." Often the better move is to titrate down to a maintenance dose, not stop entirely (which risks rebound weight gain).
Frequently Asked Questions
Is Ozempic face permanent? Not entirely. Skin and subcutaneous fat partially recover over 6–12 months after weight stabilizes, especially in younger patients.
At what weight loss does it appear? Most people notice it around 15–20 lb or 10–20% of starting weight. Faster losses make it appear earlier.
Can I prevent it? You can reduce severity by slowing the rate of loss, eating enough protein (1.2–1.6 g/kg/day), strength training 2–3× weekly, sleeping enough, and using daily SPF.
Will fillers fix it? They restore lost volume effectively. Best done after weight has stabilized for at least 6 months.
Does Mounjaro cause it less than Ozempic? Not pharmacologically — both class effects apply — but tirzepatide tends to produce faster and larger weight loss, which can make facial changes more pronounced.
Should I stop the GLP-1? Usually not. Lowering to a maintenance dose or adjusting protein, training, and pace is more effective than stopping.
Who coined the term "Ozempic face"? Dermatologist Dr. Paul Jarrod Frank, in 2022, to describe the rapid facial changes he was seeing in patients on these medications.
Last reviewed: May 13, 2026




