


If you have heard of GLP-1, you have probably wondered whether GLP-2 is the next-generation version — a stronger, newer, or "better" cousin. It is not. GLP-1 and GLP-2 are produced from the same precursor gene, by the same gut cells, often within the same minute after a meal — and they then do almost entirely different things in the body. Only one of them has anything to do with weight loss.
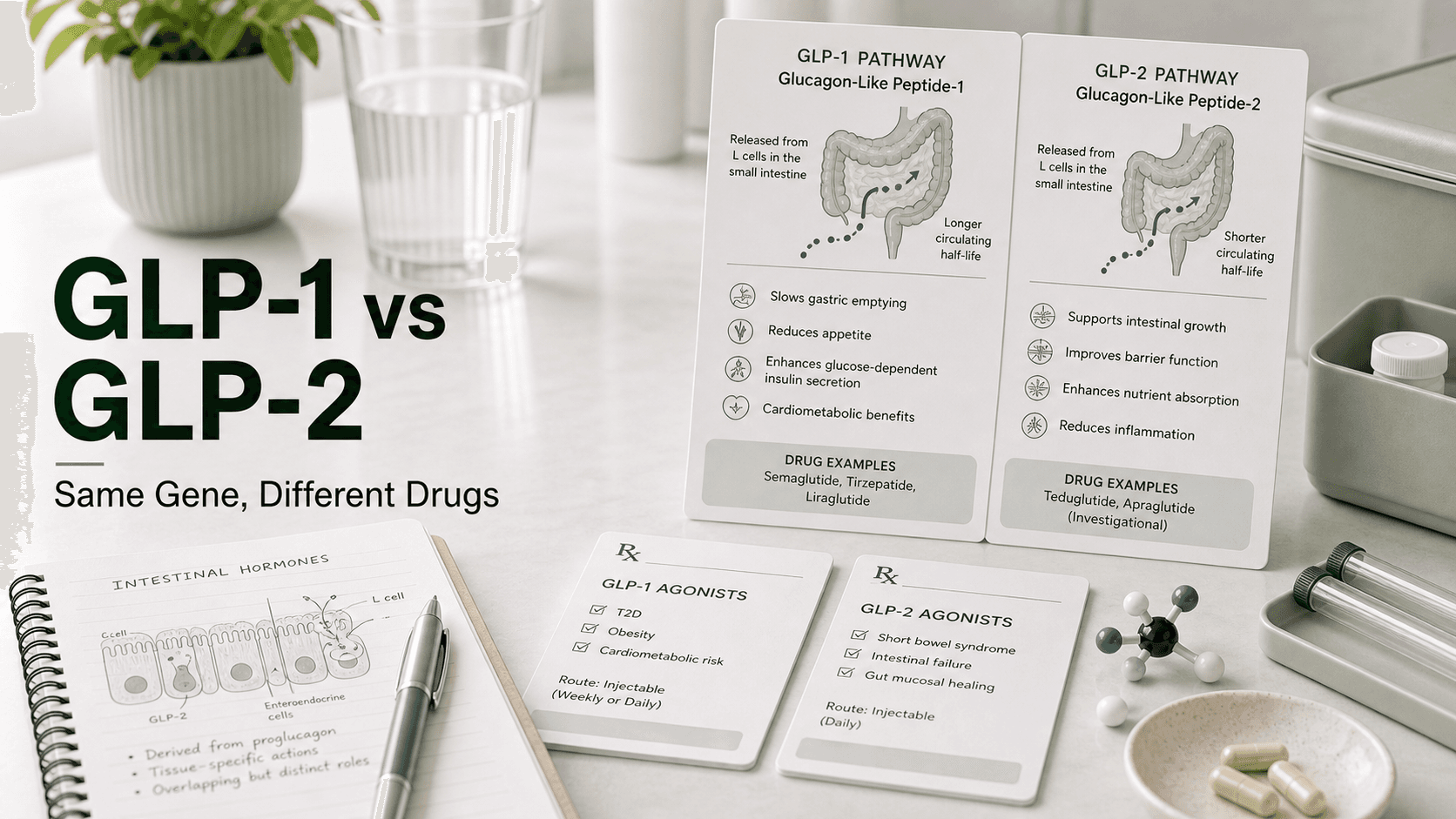
Direct answer: GLP-1 is a 30-amino-acid gut peptide that binds the GLP-1 receptor (GLP-1R) to trigger insulin release, slow gastric emptying, and suppress appetite — the basis of semaglutide, tirzepatide, liraglutide, dulaglutide, and exenatide. GLP-2 is a 33-amino-acid peptide that binds the GLP-2 receptor (GLP-2R) — found almost exclusively in the gut — to grow intestinal villi, increase nutrient absorption, and improve gut barrier function. The only FDA-approved GLP-2 drug is teduglutide (Gattex in the US, Revestive in Europe; Takeda Pharmaceuticals), indicated for short bowel syndrome (SBS) at 0.05 mg/kg/day subcutaneously. GLP-2 is not a weight-loss drug. And "GLP-3" does not exist in human physiology — it is a marketing nickname for retatrutide, a triple receptor agonist still in trials.
One Gene, Two Peptides: The Proglucagon Origin
Both peptides come from the same parent molecule: proglucagon, a 160-amino-acid precursor encoded by the GCG gene.
What happens to proglucagon depends on which cell is processing it:
- In the pancreatic alpha-cell, prohormone convertase 2 (PC2) cleaves it mostly into glucagon — the hormone that raises blood sugar.
- In the intestinal L-cell and certain brainstem neurons, prohormone convertase 1/3 (PC1/3) cleaves it into a different set of fragments: glicentin, oxyntomodulin, GLP-1, intervening peptide-2, and GLP-2.
Intestinal L-cells co-secrete GLP-1 and GLP-2 in equimolar amounts after a meal. Same cell, same trigger, same release — but two peptides with distinct receptors waiting downstream.
GLP-1 in Detail
GLP-1 is the better-known sibling. Native GLP-1(7-36) amide is 30 amino acids long, has a half-life of about 2 minutes in plasma (rapidly chewed up by DPP-4 enzyme), and binds the GLP-1 receptor (GLP-1R) — a Class B G-protein-coupled receptor widely distributed across:
- Pancreatic beta-cells
- Stomach and gut
- Hypothalamus and brainstem (appetite centers)
- Heart, kidney, and vasculature
Activating GLP-1R produces:
- Glucose-dependent insulin release — only when blood sugar is elevated
- Suppressed glucagon secretion
- Slowed gastric emptying — meals enter the bloodstream gradually
- Reduced appetite and quieted "food noise"
- Cardiovascular and renal protection (shown in SELECT, FLOW trials with semaglutide)
This is the mechanism leveraged by every GLP-1 receptor agonist on the market.
GLP-2 in Detail
GLP-2 is 33 amino acids long. Its native half-life is roughly 7 minutes — also degraded by DPP-4, but the second cleavage product is less rapidly cleared than for GLP-1. It binds the GLP-2 receptor (GLP-2R), which has a much narrower distribution than GLP-1R:
- Enteric neurons in the gut wall
- Subepithelial myofibroblasts of the small intestine
- A small population of enteroendocrine cells
- Minimal expression outside the GI tract
Activating GLP-2R does almost the opposite job of GLP-1R — it builds and protects the intestinal lining:
- Increases villus height and crypt depth — physically growing absorptive surface area
- Enhances nutrient and fluid absorption
- Strengthens gut barrier function (tight junction integrity)
- Increases intestinal and portal blood flow
- Reduces gastric acid secretion
- Modestly slows gut motility to extend absorption time
GLP-2 is not appreciably involved in insulin secretion, brain appetite signaling, or fat metabolism in any clinically meaningful way. Its receptor is simply not in the right tissues for that.
Side-By-Side
| GLP-1 | GLP-2 | |
|---|---|---|
| Amino acid length | 30 (GLP-1(7-36) amide) | 33 |
| Parent peptide | Proglucagon | Proglucagon |
| Released from | Intestinal L-cells, brainstem neurons | Intestinal L-cells |
| Co-secreted with | GLP-2, oxyntomodulin | GLP-1, oxyntomodulin |
| Half-life (native) | ~2 minutes | ~7 minutes |
| Receptor | GLP-1R | GLP-2R |
| Receptor location | Pancreas, brain, gut, heart, kidney | Almost exclusively gut |
| Insulin release | Yes, strong, glucose-dependent | No |
| Appetite suppression | Strong | None of note |
| Gastric emptying | Strongly slowed | Modestly slowed |
| Intestinal villus growth | No | Yes — primary action |
| Approved drug indications | Type 2 diabetes, obesity, MASH, CV/renal risk | Short bowel syndrome |
The Drugs in Each Class
The clinical lineups look nothing alike.
GLP-1 receptor agonists (treat type 2 diabetes, obesity, and increasingly cardiovascular and renal disease):
- Semaglutide — Ozempic, Wegovy, Rybelsus (Novo Nordisk)
- Tirzepatide — Mounjaro, Zepbound (Lilly) — technically dual GLP-1/GIP, but functionally in this class
- Liraglutide — Victoza, Saxenda (Novo Nordisk)
- Dulaglutide — Trulicity (Lilly)
- Exenatide — Byetta, Bydureon (AstraZeneca)
- Plus newer entrants such as oral orforglipron and triple agonists in late-stage trials
GLP-2 receptor agonists (treat short bowel syndrome):
- Teduglutide — Gattex (US) / Revestive (EU), Takeda Pharmaceuticals
That is the entire list. Teduglutide is the only FDA-approved GLP-2 receptor agonist and has been since 2012. A few next-generation GLP-2 analogs (apraglutide, glepaglutide) are in late-stage development for the same indication, not for metabolic disease.
Teduglutide (Gattex) Specifics
Teduglutide is a 33-amino-acid analog of human GLP-2 with a single substitution — glycine for alanine at position 2 — which makes it resistant to DPP-4 cleavage. That single change extends the half-life from about 7 minutes (native) to roughly 1.3 hours in adults with SBS, enough to support once-daily subcutaneous dosing.
- Indication: Short bowel syndrome in patients 1 year and older who are dependent on parenteral support (IV nutrition or hydration)
- Dose: 0.05 mg/kg/day subcutaneously, rotating injection sites (abdomen, thigh, upper arm)
- Reduced dose: Half-dose in moderate-to-severe renal impairment
- What it does in trials: In the pivotal 24-week study, teduglutide reduced parenteral support volume requirements significantly versus placebo by enhancing absorption from the remaining intestine.
- Notable risks: Accelerated abnormal cell growth, intestinal polyps, bowel obstruction, gallbladder and pancreatic inflammation, fluid overload — distinct from the GLP-1 side effect profile.
- Cost: Among the most expensive prescription drugs in the world, typically exceeding $300,000 per year per adult patient.
This is not a drug anyone takes to lose weight. In SBS patients it can actually help maintain weight by improving absorption from a shortened intestine.
Why "GLP-2 for Weight Loss" Is Not a Thing
Searches and supplement marketing sometimes suggest GLP-2 is an alternative to GLP-1 for weight management. It is not, for three concrete reasons:
- GLP-2 receptors are barely expressed in the brain. GLP-1's appetite-suppressing punch comes from receptors in the hypothalamus and brainstem. GLP-2R is essentially a gut receptor.
- GLP-2 does not trigger insulin release. It contributes nothing to glucose-dependent insulinotropic signaling.
- GLP-2 promotes intestinal absorption. Its job is to make the gut absorb more nutrients and fluid, not less. In short bowel syndrome that is therapeutic. In metabolic disease, the directional effect is exactly the wrong sign for weight loss.
Some research has even examined whether blocking GLP-2 might assist weight regulation, given its lipid-absorption-promoting role — the opposite of "GLP-2 agonist for weight loss."
The "GLP-3" Misconception
There is no third human glucagon-like peptide. Human proglucagon produces glucagon, GLP-1, GLP-2, oxyntomodulin, and glicentin — full stop. (A peptide called "GLP-3" exists in some cartilaginous fish, with no relevance to human medicine.)
The "GLP-3" label currently circulating in compounding-pharmacy and gray-market marketing is a nickname for retatrutide (LY3437943), an investigational triple agonist that hits GLP-1, GIP, and glucagon receptors. It is not a new endogenous peptide. It is not FDA approved. The "GLP-3" framing exists because "third receptor" makes it sound like a natural progression — but retatrutide does not bind any "GLP-3 receptor," because no such receptor exists.
What People Get Wrong
- "GLP-2 is the upgraded version of GLP-1." Different receptor, different target organ, different disease.
- "Teduglutide is a weight-loss drug." It is an absorption-enhancing drug for short bowel syndrome.
- "GLP-1 and GLP-2 do roughly the same things." They share a precursor and a release trigger. Their downstream effects barely overlap.
- "GLP-3 is the next generation after GLP-2." GLP-3 does not exist in human biology. The label is marketing for retatrutide.
- "You can stack a GLP-2 with semaglutide for better results." There is no clinical evidence base for this in healthy or obese people, and teduglutide carries serious risks including polyp formation.
Frequently Asked Questions
What is the difference between GLP-1 and GLP-2? GLP-1 (30 amino acids) acts on GLP-1 receptors in the pancreas, brain, and gut to trigger insulin release, slow gastric emptying, and reduce appetite. GLP-2 (33 amino acids) acts on GLP-2 receptors found almost exclusively in the gut to grow intestinal villi and increase nutrient absorption.
Are GLP-1 and GLP-2 the same hormone? No. They are two different peptides produced from the same precursor protein (proglucagon) by the same intestinal cells, but they bind distinct receptors and produce different effects.
What drugs target GLP-2? Only teduglutide (Gattex in the US, Revestive in Europe), made by Takeda. It is approved for short bowel syndrome.
Is GLP-2 used for weight loss? No. GLP-2 promotes intestinal absorption and gut growth. It is not a weight-loss mechanism.
Is GLP-3 a real peptide? Not in humans. The "GLP-3" label is a marketing nickname for retatrutide, a triple GLP-1/GIP/glucagon receptor agonist still in clinical trials. There is no human GLP-3 receptor.
Can I take semaglutide and teduglutide together? There is no established clinical use case for combining the two, and teduglutide has serious risks (polyps, bowel obstruction, pancreatitis) that make off-label combination a poor idea. Talk to your prescriber.
Why is teduglutide so expensive? It is an orphan drug for a rare disease (short bowel syndrome). Annual cost in the US typically exceeds $300,000.
Last reviewed: May 13, 2026
Sources
- GLP-1 vs GLP-2: Two Different Peptides Explained — PlexusDx
- A comparison of glucagon-like peptides 1 and 2 — PubMed
- How GATTEX (teduglutide) Works — Takeda
- GATTEX Dosing and Administration — Takeda
- Gattex (teduglutide) — Medscape Reference
- Proglucagon-Derived Peptides: Mechanisms and Therapeutic Potential — American Physiological Society
- Physiology of Proglucagon Peptides — Physiological Reviews
- Use of teduglutide in adults with SBS-associated intestinal failure — Nutrition in Clinical Practice (Wiley)
- A unique hormonal recognition feature of the human GLP-2 receptor — Cell Research / Nature




