


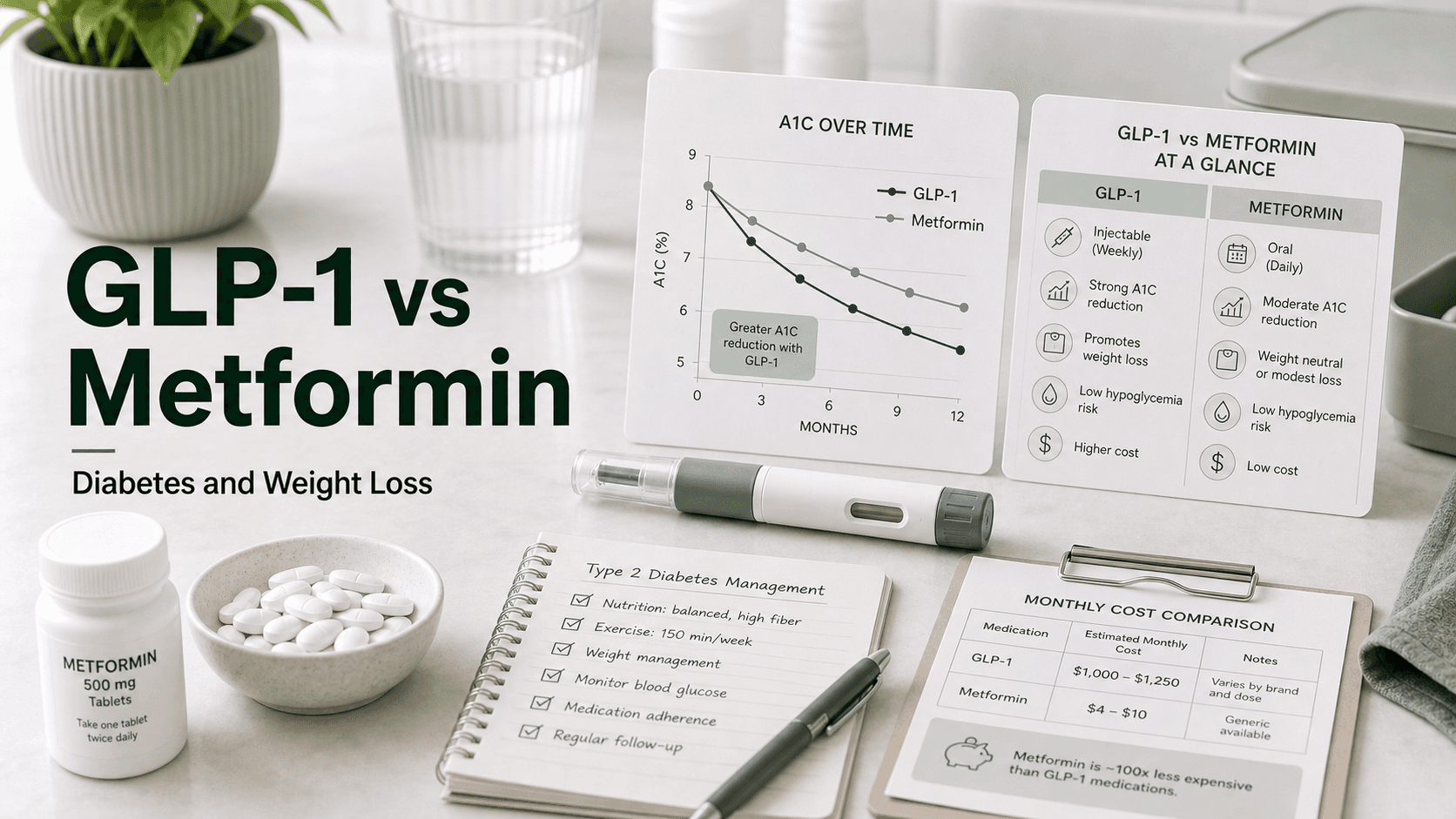
Metformin has been the default first pill for type 2 diabetes for almost 30 years. It is dirt cheap, well understood, and works. GLP-1 receptor agonists are newer, drop A1C harder, and produce dramatically more weight loss — but they cost up to 300 times as much per month and rely on weekly injections. The honest answer is that this is rarely a true either/or decision: most patients end up taking both, because they treat type 2 diabetes through completely different mechanisms.
Direct answer: Metformin lowers blood sugar by reducing how much glucose the liver pumps out and by making muscle and fat tissue more sensitive to insulin. It produces ~1.0-1.5% A1C reduction and ~2-5 lb of weight loss, for ~$4-10 per month as a generic pill. GLP-1 receptor agonists (semaglutide, tirzepatide, liraglutide) mimic an incretin hormone, triggering glucose-dependent insulin release, slowing gastric emptying, and quieting appetite. They produce ~1.5-2.5% A1C reduction and ~15-20% weight loss, for ~$0-1,300 per month depending on insurance. The 2025 ADA Standards of Care still list metformin as a foundational drug, but now recommend a GLP-1 RA or dual GIP/GLP-1 RA as the first-choice drug for patients whose diabetes is paired with overweight or obesity — which is most of them.
GLP-1 and Metformin Side By Side
| Metformin | GLP-1 RA (semaglutide) | Dual GIP/GLP-1 (tirzepatide) | |
|---|---|---|---|
| Drug class | Biguanide | Incretin mimetic | Dual incretin mimetic |
| FDA approval | 1995 (US) | 2017 (Ozempic) | 2022 (Mounjaro) |
| Form | Oral pill | Weekly injection (or daily pill) | Weekly injection |
| Typical dose | 500-2,000 mg/day | 0.25-2.4 mg/week | 2.5-15 mg/week |
| A1C reduction | 1.0-1.5% | 1.5-1.8% | 2.0-2.5% |
| Weight loss | 2-5 lb (1-3%) | ~15% (SUSTAIN/STEP) | ~20% (SURPASS/SURMOUNT) |
| Cost (cash, US) | $4-10/month generic | $0-1,300/month | $0-1,200/month |
| Hypoglycemia risk alone | Very low | Very low | Very low |
| Cardiovascular benefit | Modest | Proven (SUSTAIN-6, SELECT) | Pending (SURPASS-CVOT) |
| FDA-approved for weight loss | No (off-label) | Yes (Wegovy) | Yes (Zepbound) |
| First-line in ADA 2025? | Yes (still foundational) | Yes (if weight or CV risk is a concern) | Yes (if weight is a primary concern) |
The most important row is the last one. The ADA stopped treating metformin as the mandatory first step in 2023, and the 2025 guidance is even more permissive — a GLP-1 RA or tirzepatide can be the first drug if weight loss, cardiovascular risk reduction, or kidney protection is a priority.
How Metformin Actually Works
Metformin is the only widely used biguanide, and despite 60+ years in clinical use, its full mechanism is still being mapped. The accepted mechanism has three layers:
- Suppresses hepatic glucose production. The liver normally drips glucose into the bloodstream between meals and overnight. In type 2 diabetes, this drip is excessive. Metformin reduces it, lowering fasting blood sugar significantly.
- Improves insulin sensitivity in muscle and fat. Metformin makes existing insulin work better, partly through activating AMP-activated protein kinase (AMPK).
- Slows intestinal glucose absorption and modestly increases gut GLP-1 release — which is why some of metformin's benefit overlaps with the GLP-1 drugs.
It does not stimulate insulin secretion, which is why metformin alone almost never causes hypoglycemia. Blood sugar can only go as low as the body's own counter-regulatory hormones allow.
How GLP-1 Receptor Agonists Actually Work
GLP-1 (glucagon-like peptide-1) is an incretin hormone secreted by gut L-cells in response to food. Its native half-life is about 2 minutes, which is why it took protein engineering to turn it into a usable drug. GLP-1 RAs are modified peptides that resist the enzyme DPP-4 and circulate for hours to days.
Activating the GLP-1 receptor:
- Triggers glucose-dependent insulin release from the pancreas — only when blood sugar is high
- Slows gastric emptying so meals enter the bloodstream gradually
- Suppresses glucagon so the liver does not dump glucose
- Quiets food noise — intrusive thoughts about food driven by the hypothalamus
- Reduces caloric intake by 20-35% in clinical trial settings
- May protect heart and kidney tissue (SUSTAIN-6, SELECT, FLOW outcome trials)
Tirzepatide adds a second receptor — GIP — which appears to soften the nausea that limits semaglutide and to directly improve fat-tissue insulin sensitivity. See our GLP-1 and GIP deep dive for the receptor-level pharmacology.
A1C Reduction: GLP-1 Wins, But Not By As Much As You'd Think
Across head-to-head trials and meta-analyses, the spread is real but smaller than the marketing implies.
| Drug | A1C reduction at max dose | Trial reference |
|---|---|---|
| Metformin 2,000 mg | ~1.0-1.5% | Decades of monotherapy studies |
| Liraglutide 1.8 mg | ~1.0-1.5% | LEAD program |
| Semaglutide 1 mg | ~1.5-1.8% | SUSTAIN program |
| Semaglutide 2 mg | ~1.8-2.2% | SUSTAIN FORTE |
| Tirzepatide 15 mg | ~2.0-2.5% | SURPASS program |
A Danish nationwide cohort study of drug-naive patients found GLP-1 RA first-line therapy produced ~2.6-3.8 mmol/mol greater A1C drop than metformin first-line, and a 33% lower risk of needing add-on therapy at 1 year for diabetic patients (relative risk 0.67).
The numbers are honest but the bigger truth is that for many newly diagnosed patients, metformin alone can bring A1C below 7% if started early. The case for a GLP-1 over metformin gets stronger as starting A1C climbs and as BMI climbs.
Weight Loss: This Is Where the Gap Is Enormous
Metformin produces modest, real weight loss — typically 2-5 lb over the first six months, or roughly a 2-3% body weight reduction. The mechanism appears to involve mild appetite suppression and gut microbiome shifts, not just glucose control.
GLP-1 drugs are in a completely different category:
| Drug | Average weight loss at top dose | Trial |
|---|---|---|
| Metformin 2,000 mg | 2-5 lb (~2-3%) | Diabetes Prevention Program |
| Liraglutide 3 mg (Saxenda) | ~6% at 56 weeks | SCALE |
| Semaglutide 2.4 mg (Wegovy) | ~15% at 68 weeks | STEP-1 |
| Tirzepatide 15 mg (Zepbound) | ~21% at 72 weeks | SURMOUNT-1 |
That is roughly a 5-10x weight-loss advantage for high-dose GLP-1 drugs versus metformin. For a 220 lb patient, the gap is 5 lb on metformin versus 33-46 lb on semaglutide or tirzepatide.
Metformin's weight-loss reputation is solid but oversold. It is a metabolic helper, not a weight-loss drug.
What the 2025 ADA Standards Actually Say
The 2025 ADA Standards of Care updated the algorithm for type 2 diabetes pharmacotherapy with a clearer hierarchy:
- Metformin is still endorsed as a foundational, low-cost, well-tolerated option, especially when cost is a barrier and weight is not a primary concern.
- For patients with type 2 diabetes and overweight/obesity, the ADA now recommends a GLP-1 RA or a dual GIP/GLP-1 RA with high weight-loss potential (semaglutide or tirzepatide) as the first-choice pharmacological treatment.
- For patients with established atherosclerotic cardiovascular disease, heart failure, or chronic kidney disease, an SGLT2 inhibitor or GLP-1 RA with demonstrated cardiorenal benefit is recommended — independent of A1C.
- When metformin alone is insufficient, adding a GLP-1 RA or GIP/GLP-1 RA typically yields another 1 to ≥2% A1C reduction.
- The ADA explicitly says do not combine a GLP-1 RA with a DPP-4 inhibitor — same pathway, no added benefit.
The net: metformin is no longer the legally required first step, but it remains the most cost-effective default when nothing else dictates a different choice.
Side Effect Profiles: Both Hit the Gut, Differently
Both classes are dominated by GI side effects. The timing and texture differ.
| Side effect | Metformin | Semaglutide |
|---|---|---|
| Nausea | 7-25% (improves with dose splitting) | 15-44% (worst during titration) |
| Diarrhea | 30-53% (often persistent) | 8-30% |
| Vomiting | Rare | 5-25% |
| Bloating, gas | Common, often persistent | Common, often transient |
| Hypoglycemia (alone) | <1% | <1% |
| Vitamin B12 deficiency | ~10-30% with long-term use | None |
| Lactic acidosis | Very rare (<10/100,000) | None |
| Pancreatitis signal | None | Rare but tracked |
| Gallbladder issues | None | Slightly increased |
| Thyroid C-cell concern | None | Boxed warning (rodent data) |
Metformin's diarrhea is often the deal-breaker. Extended-release formulations cut it down significantly. GLP-1 nausea typically improves after the first 4-8 weeks at each dose if titration is slow.
Cost: This Is the Real Decision Driver for Many Patients
This is where the comparison stops being subtle.
| Drug | Cash price (US, generic where available) | With commercial insurance | Without coverage |
|---|---|---|---|
| Metformin IR generic | $4-10/month | $0-5 copay | $4-10 |
| Metformin ER generic | $10-25/month | $0-10 copay | $10-25 |
| Ozempic (semaglutide) | $968/month list | $25-250 with copay card | $700-1,000 |
| Wegovy (semaglutide 2.4) | $1,349/month list | $0-25 with savings card | $500 (NovoCare direct cash) |
| Mounjaro (tirzepatide) | $1,069/month list | $25 with savings card | $349-499 (LillyDirect cash) |
| Zepbound (tirzepatide) | $1,086/month list | $25 with savings card | $349-499 (vial program) |
| Compounded semaglutide | Roughly $150-300/month from licensed pharmacies | Out of pocket | Out of pocket |
A year of metformin generic costs ~$50. A year of brand-name Wegovy at list price is ~$16,000. That is a 300-fold spread and it explains why many patients start metformin and only escalate to a GLP-1 when insurance covers it or when the clinical case is strong enough to justify out-of-pocket spend.
Drug Interactions Worth Knowing
Metformin:
- Iodinated contrast dye — hold metformin around imaging studies; risk of lactic acidosis if kidney function drops.
- Heavy alcohol — same lactic acidosis concern.
- Carbonic anhydrase inhibitors (topiramate, acetazolamide) — additive acidosis risk.
- Cimetidine, ranolazine, dolutegravir — raise metformin levels.
GLP-1 RAs:
- Sulfonylureas and insulin — hypoglycemia risk goes up sharply; sulfonylurea dose typically gets cut by 25-50% when starting a GLP-1.
- Oral medications with narrow therapeutic windows (warfarin, levothyroxine, hormonal contraceptives) — delayed gastric emptying can shift absorption.
- DPP-4 inhibitors — no added benefit, do not combine.
Crucially, metformin and GLP-1 RAs have no meaningful interactions with each other and are very commonly used together.
Combination Therapy Is the Norm, Not the Exception
This is the part the "vs" framing hides. In real clinical practice, most patients prescribed a GLP-1 are already on metformin and stay on it. The mechanisms complement rather than overlap:
- Metformin addresses hepatic glucose output and insulin sensitivity — supply side.
- GLP-1 addresses post-meal insulin release, gastric emptying, and appetite — demand side.
Combination data:
- Semaglutide added to metformin produces another ~1.1-1.8% A1C reduction beyond metformin alone.
- Weight loss with the combination is typically slightly greater than semaglutide alone in trials.
- Cancer incidence data suggest dual metformin + GLP-1 RA use is associated with ~39% lower adiposity-related cancer incidence and lower all-cause mortality versus either drug alone (observational).
- GI side effects can stack — most clinicians slow GLP-1 titration in patients on full-dose metformin.
The ADA 2025 algorithm assumes combination therapy from the start for many patients, not sequential monotherapy.
Who Is Best Suited for Each
Metformin first makes sense when:
- A1C is mildly elevated (7.0-8.0%) and BMI is normal or near-normal
- Cost is a primary concern and a GLP-1 cannot be afforded or covered
- The patient prefers oral medication and has no GI red flags
- Kidney function is adequate (eGFR ≥30)
- There is no current cardiovascular or kidney disease driving a specific drug class choice
A GLP-1 RA first (or added early) makes sense when:
- A1C is high (>8.5%) at diagnosis
- BMI is ≥27 and weight loss is a therapeutic goal
- Established ASCVD, heart failure with reduced ejection fraction, or CKD
- The patient has tried metformin and hit GI intolerance or insufficient response
- Cost coverage is in place via insurance, manufacturer savings, or direct cash programs
Tirzepatide specifically moves to first-line consideration when weight loss is the dominant clinical priority and SURPASS-style A1C drops (~2.5%) are needed.
Switching from Metformin to a GLP-1
In practice, "switching" is rarely all-or-nothing. The typical pattern:
- Continue metformin during GLP-1 initiation. The combination is the goal, not the stepping stone.
- Start the GLP-1 at the lowest dose (semaglutide 0.25 mg/week or tirzepatide 2.5 mg/week) for at least 4 weeks before any increase.
- Monitor A1C at 3 months. If at target, stay there. If not, escalate the GLP-1, not the metformin.
- Reassess metformin only if GI side effects are unmanageable, kidney function drops, or A1C is at or below 6.5% on the combination and de-escalation is reasonable.
- Never stop metformin abruptly in a patient with established T2D — A1C tends to climb within 8-12 weeks.
If cost or tolerability forces a choice between the two long-term, the question becomes whether weight loss or glycemic-mechanism breadth matters more. For many patients with T2D plus obesity, the GLP-1 wins both fights.
What People Get Wrong About GLP-1 vs Metformin
- "Metformin is obsolete now that we have Ozempic." Not true. Metformin remains foundational in the 2025 ADA Standards, costs almost nothing, and adds independent benefit to a GLP-1.
- "GLP-1s only work for weight loss." Semaglutide and tirzepatide are FDA approved for type 2 diabetes; weight loss is a side effect of the same mechanism.
- "You can replace metformin with berberine." Berberine has weak comparative data and is not FDA approved. Metformin is still cheaper and far better studied.
- "You can't take both at the same time." You almost always can, and most patients do. There is no pharmacokinetic interaction.
- "GLP-1s cure diabetes." They control it. Stopping the drug returns A1C and weight to baseline in most patients within months.
- "Metformin causes hypoglycemia." Alone, no. Combined with insulin or sulfonylureas, yes.
- "All GLP-1s are equally strong as metformin." Liraglutide is roughly metformin-equivalent on A1C. Semaglutide and tirzepatide are stronger.
Frequently Asked Questions
Is metformin or a GLP-1 better for type 2 diabetes? For pure A1C reduction, GLP-1 RAs (especially tirzepatide) win at the high end of dosing. For cost, simplicity, and decades of safety data, metformin wins. The 2025 ADA position is that both are appropriate first-line options depending on the patient.
Can you take metformin and Ozempic together? Yes. This is one of the most common combinations in type 2 diabetes management. They work through different mechanisms and have no clinically significant interaction. GI side effects can be additive.
Will I lose more weight on metformin or semaglutide? Semaglutide produces roughly 3-5x more weight loss than metformin in head-to-head and parallel trial data — typically 12-15% body weight versus 2-3% body weight.
Is metformin first-line in 2025? Metformin remains a recommended first-line option, but the ADA 2025 Standards explicitly allow GLP-1 RAs or tirzepatide as first-line when weight management is a goal or when ASCVD, heart failure, or CKD is present.
Why is metformin so much cheaper than a GLP-1? Metformin lost patent protection decades ago and is a small molecule, easy to manufacture. GLP-1 RAs are engineered peptides, still under patent, and require injection-grade manufacturing.
Can a GLP-1 replace metformin? Clinically, yes — many patients eventually use a GLP-1 as monotherapy when metformin is poorly tolerated. But the 2025 ADA guidance and observational data both favor keeping metformin on board unless there is a reason to drop it.
Which one has fewer side effects? Both hit the gut. Metformin causes more diarrhea overall. GLP-1s cause more nausea, especially during titration. Long-term, both are generally well tolerated by patients who get through the first 8-12 weeks.
Does metformin work for weight loss without diabetes? Modestly. Studies in non-diabetic adults show 2-6 lb weight loss over 6-12 months — real but small. It is sometimes used off-label for PCOS and prediabetes.
Last reviewed: May 13, 2026
Sources
- Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes 2025 — ADA
- Comparing GLP-1 receptor agonists versus metformin in drug-naive patients: A nationwide cohort study — Journal of Diabetes
- GLP-1 receptor agonists versus metformin nationwide cohort study — PMC
- 8 Major Differences Between Ozempic and Metformin — GoodRx
- How do Ozempic and Metformin compare for diabetes? — Drugs.com
- Metformin vs. semaglutide: A detailed comparison for weight loss and diabetes — NiceRx
- Efficacy and safety of semaglutide combined with metformin in T2DM with overweight or obesity — PMC
- Diabetes Medications as Monotherapy or Metformin-Based Combination Therapy — Annals of Internal Medicine
- Synergistic associations of metformin and GLP-1 receptor agonist use with adiposity-related cancer incidence — Diabetes, Obesity and Metabolism
- Metformin vs. GLP-1 Receptor Agonists: Which Diabetes Medication Is Right for You? — HealthCentral
- Ozempic vs. metformin: Differences, similarities, and which one is better — SingleCare




