If two GLP-1 drugs are both effective, the one that lets you stay on therapy wins. Tolerability is what drives real-world outcomes, because the drug you quit at month three does not produce weight loss at month eighteen. The good news in 2026 is that the GLP-1 with the best efficacy is also, somewhat counterintuitively, the one with the lowest trial discontinuation rate at top dose.
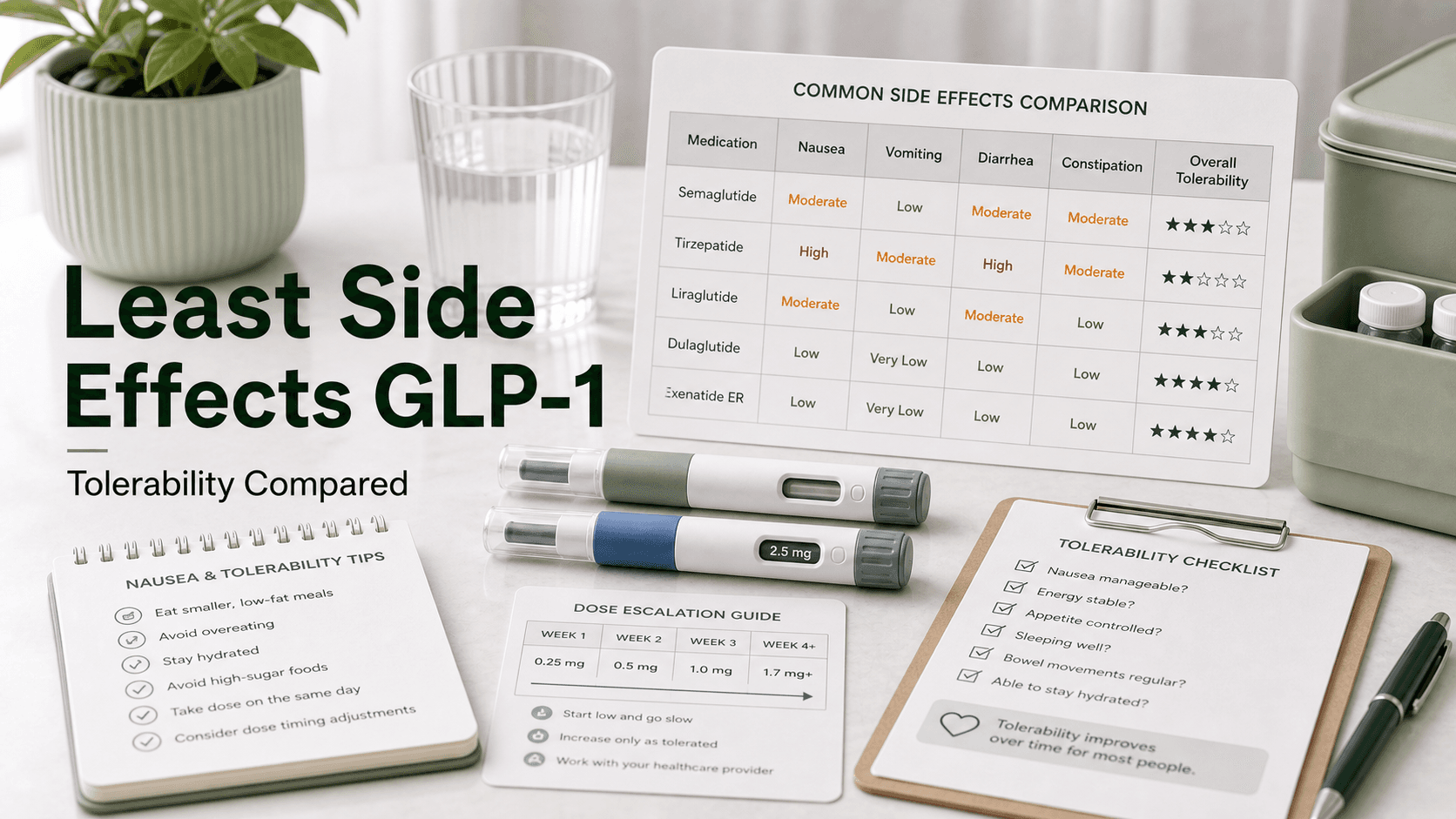
Direct answer: Among FDA-approved GLP-1 receptor agonists, tirzepatide (Zepbound, Mounjaro) has the lowest trial discontinuation rate at high dose — 3.0 to 6.6% in the SURMOUNT and SURPASS programs. Semaglutide (Wegovy, Ozempic) sits at ~7%, oral semaglutide at ~9.7%, orforglipron at ~9%, and liraglutide (Saxenda) at ~10%. Per-event GI rates tell the same story: tirzepatide produces less nausea (31.0%), less vomiting (12.2%), and slightly less diarrhea (23.0%) than semaglutide 2.4 mg (44.2% / 24.8% / 31.5%) at top dose. The GIP component appears to soften the nausea ceiling. Slower titration helps every drug.
Side Effect Comparison at Top Approved Dose
| Drug | Nausea | Vomiting | Diarrhea | Trial discontinuation |
|---|---|---|---|---|
| Tirzepatide 15 mg (SURMOUNT-1) | 31.0% | 12.2% | 23.0% | 3.0–6.6% |
| Semaglutide 2.4 mg (STEP-1) | 44.2% | 24.8% | 31.5% | ~7.0% |
| Oral semaglutide 25 mg (OASIS-1) | ~38% | ~21% | ~28% | ~9.7% |
| Orforglipron 36 mg (ATTAIN-1) | 33.7% | ~15% | ~22% | ~9% (any AE) |
| Liraglutide 3.0 mg (SCALE) | 40.2% | 16.3% | 20.9% | ~10% |
Rates are pulled from each drug's pivotal weight-loss trial. They are not perfectly head-to-head — patient populations and dose-escalation schedules differ — but the pattern is consistent across the SURMOUNT-5 head-to-head comparison and several 2025 meta-analyses.
Why Tirzepatide Is Better Tolerated at High Doses
This is the part most patients find counterintuitive. Tirzepatide is the more potent drug. It produces more weight loss than semaglutide. It would be reasonable to expect it to produce more nausea. It does not — at least not at the top doses.
The leading mechanistic explanation is the GIP (glucose-dependent insulinotropic polypeptide) component. Tirzepatide is a dual GLP-1 and GIP receptor agonist. Semaglutide is GLP-1 only. GIP receptor activation appears to dampen the nausea signal driven by GLP-1. Animal models show that GIP agonism attenuates the conditioned taste aversion that GLP-1 monotherapy produces. In humans, the practical result is that tirzepatide users can climb to a 15 mg dose with a lower peak nausea rate than semaglutide users hit at 2.4 mg.
This does not make tirzepatide nausea-free. It just lowers the ceiling. Roughly one in three tirzepatide users still report nausea, and most of it lands during dose escalation.
Drug-By-Drug Tolerability
Tirzepatide (Zepbound, Mounjaro)
- Nausea: 31.0% at 15 mg in SURMOUNT-1
- Vomiting: 12.2%
- Diarrhea: 23.0%
- Constipation: 11.7%
- Discontinuation: 3.0–6.6% across SURMOUNT and SURPASS trials
Tirzepatide's side effect profile is concentrated in the first 12 weeks of titration. Most patients who tolerate the 2.5 mg → 5 mg → 7.5 mg climb do not have severe issues at 10 mg or 15 mg. The dual-receptor mechanism appears to give it the lowest discontinuation rate of any high-efficacy GLP-1.
Semaglutide (Wegovy, Ozempic)
- Nausea: 44.2% at 2.4 mg in STEP-1
- Vomiting: 24.8%
- Diarrhea: 31.5%
- Constipation: 23.4%
- Discontinuation: ~7%
Semaglutide has the largest real-world dataset of any GLP-1. The side-effect numbers above are higher than tirzepatide's at the top dose, but most events are mild to moderate and transient. The 7% discontinuation rate is the standard most other GLP-1s are measured against.
Oral Semaglutide (Wegovy oral tablets, Rybelsus)
- Nausea: ~38% at 25 mg
- Vomiting: ~21%
- Diarrhea: ~28%
- Discontinuation: ~9.7%
The oral form has slightly lower peak plasma concentrations than the injection, which should — in theory — produce less GI burden. In practice, discontinuation is higher than the injection, likely because the empty-stomach dosing rule and the 30-minute post-dose fast are easy to break, which triggers spikes in absorption and worse symptoms.
Orforglipron (Foundayo)
- Nausea: 33.7% at 36 mg in ATTAIN-1
- Vomiting: ~15%
- Diarrhea: ~22%
- Constipation: ~24%
- Discontinuation: ~9% for any adverse event; 3.5–7% for GI specifically
Orforglipron is a non-peptide, small-molecule GLP-1 agonist. It does not require the SNAC absorption enhancer that oral semaglutide uses, and there is no food or water restriction. Per-event nausea rates look comparable to liraglutide and lower than injectable semaglutide, but the overall discontinuation rate runs higher than tirzepatide. It is a reasonable pick for needle-averse patients who want flexibility.
Liraglutide (Saxenda, Victoza)
- Nausea: 40.2% at 3.0 mg in SCALE
- Vomiting: 16.3%
- Diarrhea: 20.9%
- Constipation: 20.0%
- Discontinuation: ~10%
Liraglutide is the original obesity GLP-1, and it has the highest discontinuation rate among approved options. Two reasons: it is a daily injection (more doses, more chances to feel a side effect), and its shorter half-life means plasma levels swing more day to day. It also produces less weight loss than the newer drugs, so the side-effect-to-benefit ratio is worse.
Titration Speed Matters More Than the Drug
The single largest tolerability lever is not which GLP-1 you choose. It is how fast you climb.
A randomized comparison of semaglutide titration schedules showed that a slower, more flexible escalation cut nausea from 64% to 45% and dropped discontinuation from 19% to 2%. The standard 4-week step is convenient for clinics, but it is not a biological requirement. Many patients tolerate the drug far better when each step lasts 6 to 8 weeks instead of 4.
If your prescriber is flexible, ask about:
- Holding at 2.5 mg tirzepatide or 0.25 mg semaglutide for 8 weeks instead of 4
- Stepping back down one level if a new dose triggers severe symptoms
- Microdose escalation, which moves up in smaller increments using compounded vials
- Pausing the climb at the dose where you are getting weight-loss results, instead of pushing to the top
The dose that works is the dose you tolerate. There is no medal for reaching 15 mg.
Strategies That Reduce Side Effects on Any GLP-1
These work across every drug in the class.
- Eat slowly and stop earlier than you used to. Delayed gastric emptying means your "full" signal arrives 10 to 20 minutes later than before the drug. Stop at "not hungry" — not "full."
- Smaller, more frequent meals. Three big meals are harder to tolerate than five small ones during the first eight weeks.
- Cut fat and fried foods temporarily. High-fat meals sit in the stomach longer and trigger the worst nausea.
- Protect protein and electrolytes. Aim for 0.7 to 1.0 g of protein per pound of goal body weight, and use an electrolyte mix (sodium, potassium, magnesium) if you are losing weight quickly.
- Hydrate aggressively. Two to three liters of water per day prevents constipation and reduces the headache and fatigue that mimic side effects.
- Use ginger, peppermint, or vitamin B6 for breakthrough nausea. None will dissolve a 44% baseline rate, but they take the edge off acute episodes.
- Inject at night. Sleeping through the first 12 hours of peak plasma exposure helps many patients.
- Don't skip the dose after a bad week. Skipping resets your tolerance and makes the next dose feel worse. Lower the dose or extend the interval instead.
How to Choose if You Are Side-Effect-Sensitive
For patients with a history of bad GI tolerance — IBS, gastritis, prior chemotherapy nausea, or motion sickness — the priority order shifts.
First choice: tirzepatide at slow titration. Lowest peak nausea ceiling, lowest trial discontinuation, dual-receptor mechanism. Hold each step 6 to 8 weeks. Stop at the lowest effective dose.
Second choice: oral semaglutide at the lowest effective dose. The lower-dose tablet (3 mg or 7 mg Rybelsus) is genuinely gentle. The downside is the empty-stomach rule.
Third choice: orforglipron at the lowest effective dose. A reasonable pick if you cannot do injections and cannot follow the empty-stomach rule for oral semaglutide.
Avoid as first-line: liraglutide. The shorter half-life and daily dosing make it the worst choice for a sensitive patient when better-tolerated options exist.
What People Get Wrong
- "Tirzepatide must have more side effects because it works harder." Wrong. The dual-receptor mechanism actually softens the nausea ceiling. Tirzepatide has the lowest discontinuation rate of the high-efficacy options.
- "Liraglutide is the gentlest because it is older." Wrong. Liraglutide has the highest discontinuation rate among approved options.
- "Oral GLP-1s are always milder." Sometimes. Oral semaglutide at 25 mg has nausea rates close to the injection. Lower-dose Rybelsus is genuinely mild.
- "If I get nausea, the drug is wrong for me." Usually wrong. Nausea is overwhelmingly a titration problem, not a drug-selection problem. Slow down before switching.
- "Switching drugs will fix my side effects." Sometimes. More often, you carry the same symptom over to the new drug because the underlying issue is titration speed, eating pattern, or hydration.
Frequently Asked Questions
What GLP-1 has the least side effects? Tirzepatide (Zepbound, Mounjaro) has the lowest trial discontinuation rate among high-efficacy options — 3.0 to 6.6% in SURMOUNT and SURPASS — and the lowest top-dose nausea rate (31.0%) compared with semaglutide (44.2%) and liraglutide (40.2%).
Is Ozempic or Mounjaro easier on the stomach? Mounjaro (tirzepatide). At comparable weight-loss doses, tirzepatide produces less nausea, less vomiting, and slightly less diarrhea than Ozempic (semaglutide), with a lower trial discontinuation rate.
Which GLP-1 causes the least nausea? Tirzepatide at top dose (31.0%) and low-dose Rybelsus (~10–15%) are the lowest among commonly prescribed options. Liraglutide (40.2%) and semaglutide 2.4 mg (44.2%) sit higher.
Are oral GLP-1s gentler than injections? Sometimes. Lower-dose oral semaglutide (Rybelsus 3 mg, 7 mg) is genuinely mild. Higher-dose oral semaglutide (25 mg) and orforglipron 36 mg produce nausea rates close to or above the injectable versions.
Why does tirzepatide have less nausea than semaglutide? The leading explanation is the GIP receptor component. GIP activation appears to dampen the nausea signal driven by GLP-1, lowering the ceiling at high doses.
How can I reduce GLP-1 side effects without switching drugs? Slow your titration (6 to 8 weeks per step), eat smaller meals, cut fat temporarily, hydrate, inject at night, and stop at the lowest dose that produces weight loss instead of climbing to the top.
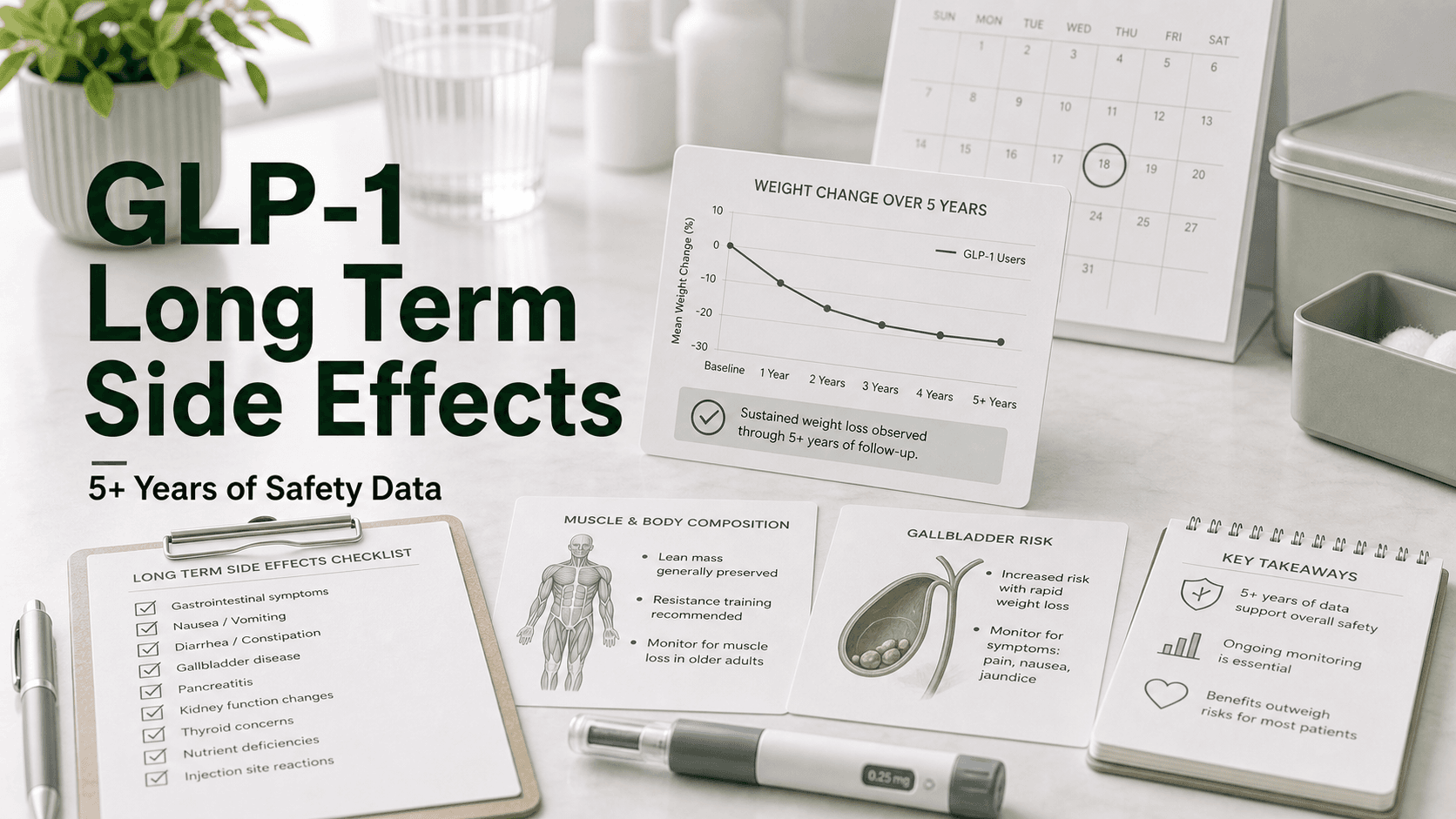
Does the side effect profile improve over time? Yes. Most GI symptoms peak during dose escalation and fade within 4 to 12 weeks at a stable dose. Patients who push through the first three months usually do not have lasting issues.
Last reviewed: May 13, 2026
Sources
- GLP-1 Side Effects Compared — Which Has Fewest?
- TrimRX: Which GLP-1 Has the Least Side Effects? A 2026 Analysis
- Comparative gastrointestinal adverse effects of GLP-1 receptor agonists (Bayesian network meta-analysis, PMC)
- Glucagon-like Receptor-1 agonists for obesity: weight loss, tolerability, side effects (PMC)
- GI adverse events and weight reduction in tirzepatide SURPASS trials (Patel et al., 2024)
- PeptideDeck: GLP-1 Side Effects Compared (Retatrutide vs Tirzepatide vs Semaglutide, 2026)
- Orforglipron Phase 3 ATTAIN-1 results (NEJM, 2025)
- SheMed: Which GLP-1 Has the Least Side Effects (UK)