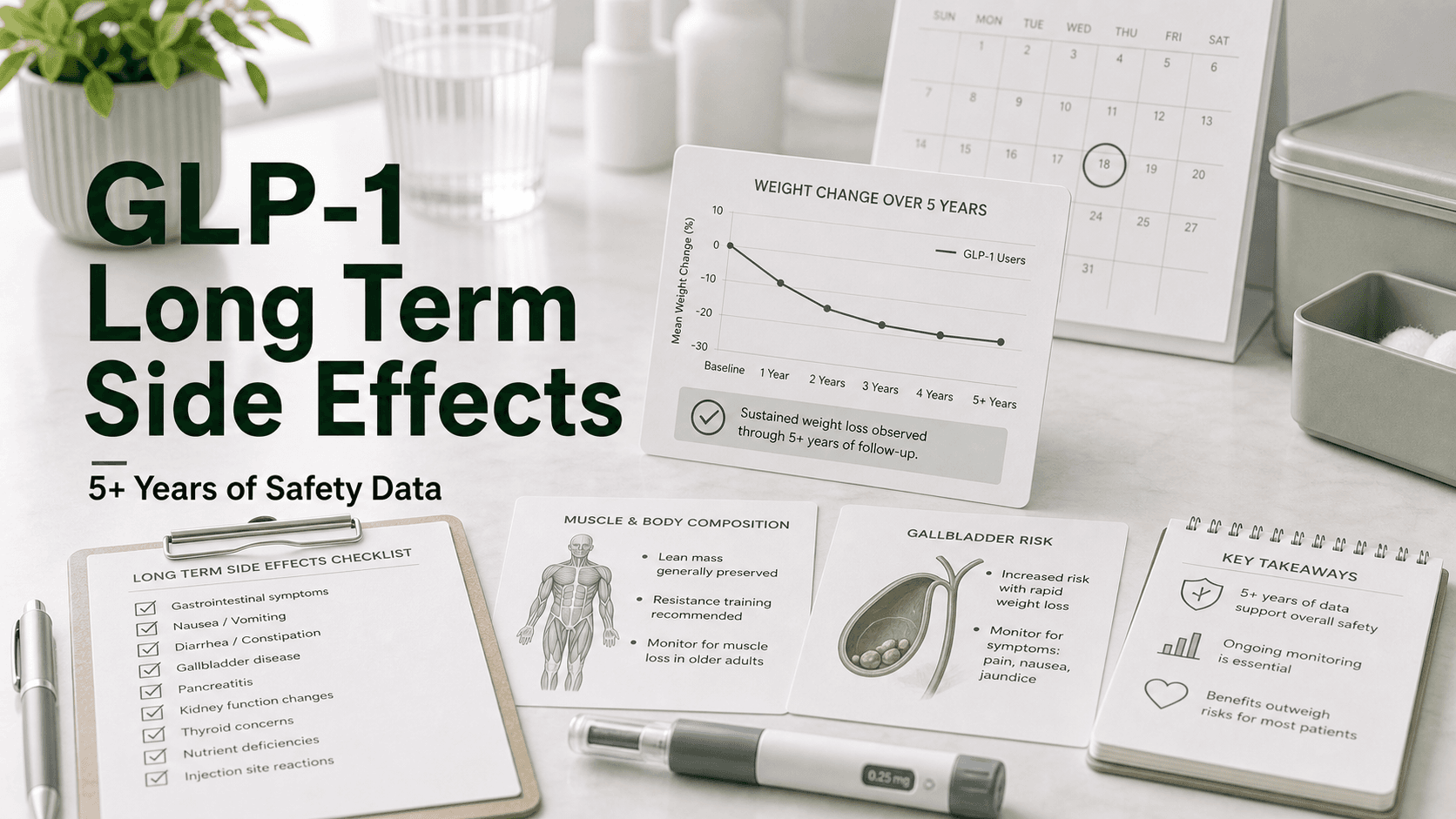
The short-term GLP-1 side effects are well-known by now: nausea, constipation, sulfur burps, fatigue during titration. The longer-term picture is what most patients actually care about, because most who tolerate the first 3 months stay on the drug indefinitely. After 5+ years of real-world semaglutide use and 3+ years of tirzepatide, plus the SELECT, FLOW, and SURMOUNT outcome trials, the long-term profile is finally taking shape.
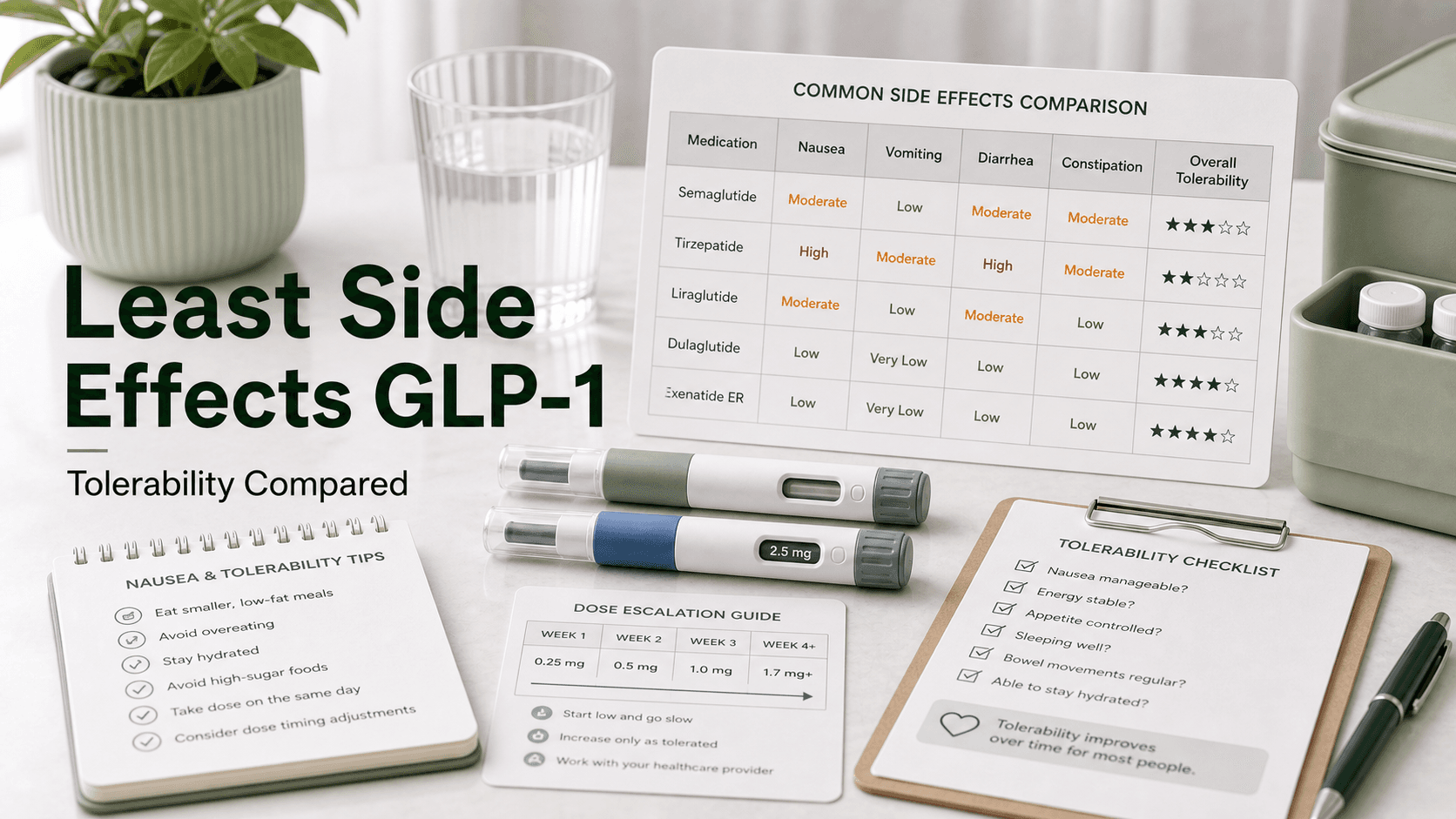
Direct answer: Most GLP-1 GI side effects fade after 3–6 months but can resurface with dose increases. Trial nausea rates by drug: liraglutide 40.2%, semaglutide 44.2%, tirzepatide 31.0%. Long-term concerns include: lean muscle loss (25–40% of total weight lost without strength training), gallbladder disease (2.6% on semaglutide vs 1.2% placebo), bone density loss (especially in post-menopausal patients), rare acute pancreatitis, the NAION vision signal for semaglutide, persistent gastroparesis in a small subset, and delayed gastric emptying that complicates anesthesia and colonoscopy. After stopping semaglutide, patients regain about 2/3 of lost weight, leaving net loss of 5.6% at 120 weeks. Thyroid C-cell tumor remains a boxed warning but is unconfirmed in humans.
GI Side Effects That Usually Fade
These dominate the first 3 months and then typically settle. Trial data from pooled obesity trials:
| Side effect | Liraglutide 3.0 mg | Semaglutide 2.4 mg | Tirzepatide 15 mg |
|---|---|---|---|
| Nausea | 40.2% | 44.2% | 31.0% |
| Diarrhea | 20.9% | 31.5% | 23.0% |
| Vomiting | 16.3% | 24.8% | 12.2% |
| Constipation | ~15% | ~24% | ~17% |
The pattern: tirzepatide produces less nausea and vomiting than semaglutide despite producing more weight loss. The GIP component appears to buffer GLP-1's nausea ceiling.
Most of these spike again briefly each time the dose is escalated, then re-settle within 1–2 weeks at the new dose.
Side Effects That Persist or Emerge Later
These shape the multi-year decision to stay on a GLP-1.
Lean Muscle Loss
Trial DEXA studies and real-world data show that 25–40% of total weight loss on a GLP-1 can come from lean mass when patients don't resistance train. Not unique to GLP-1s — happens with any rapid weight loss — but it stacks across years on the medication.
Mitigation:
- 1.2–1.6 g protein per kg of body weight per day
- Resistance training 2–3× per week, including compound lifts
- Slower titration if weight is dropping rapidly
- Periodic body composition measurement (DEXA, smart scale, InBody) to confirm fat loss dominates
Bone Density Loss
Smaller studies and bariatric surgery data suggest meaningful weight loss can reduce bone mineral density, particularly at the hip and lumbar spine. Long-term GLP-1 data is still being collected, but the trajectory likely follows other rapid weight loss.
Mitigation:
- Resistance training (impact and load)
- Adequate calcium (1,000–1,200 mg/day) and vitamin D (typically 1,000–2,000 IU/day)
- Baseline + follow-up DEXA scans for at-risk patients (post-menopausal, BMI <22 at goal, fracture history)
Gallbladder Disease
GLP-1s slow gallbladder emptying and biliary motility. Pooled trial data:
| Drug | Gallbladder disorder rate |
|---|---|
| Liraglutide | 0.8% cholelithiasis, 0.5% acute cholecystitis |
| Semaglutide | 2.6% vs 1.2% placebo |
| Tirzepatide | ≤0.6% acute cholecystitis |
A meta-analysis concluded GLP-1 receptor agonists "were linked to a higher risk of gallbladder or biliary diseases, particularly when used at higher doses." Rapid weight loss compounds the risk.
Mitigation:
- Gradual weight loss rather than rapid
- Adequate dietary fat (very low-fat diets paradoxically promote gallstones)
- Surgical consultation for right-upper-quadrant pain, nausea after fatty meals, or jaundice
Pancreatitis
Rare. Trial data:
- Liraglutide: 10 cases (9 mild, 5 gallstone-related) vs 1 placebo
- Semaglutide: 3 mild cases, all recovered, all in patients with prior pancreatitis or gallstones
- Tirzepatide: 4 cases evenly distributed across treatment and placebo, none severe
Multiple meta-analyses show "no significant difference in development of acute pancreatitis or pancreatic cancer" vs placebo overall. Risk is higher in patients with:
- Prior pancreatitis history
- Gallstones
- Heavy alcohol use
- Triglycerides over ~500 mg/dL
Symptoms (severe upper abdominal pain radiating to the back, with vomiting) warrant emergency evaluation.
Chronic Gastroparesis
The most controversial long-term signal. Most GLP-1 patients experience drug-induced delayed gastric emptying that resolves after discontinuation. A small subset develop persistent gastroparesis that lingers months or years after stopping. The MDL-3094 litigation centers on this signal.
Patients with significant pre-existing GI motility issues are at highest risk and often should not be on a GLP-1 at all.
Anesthesia and Procedure Risks
A late-emerging concern: residual gastric contents on semaglutide create aspiration risk during anesthesia. Expert consensus recommends:
- Withhold the medication for at least 3 half-lives (~88% clearance) before procedures with anesthesia
- For weekly semaglutide/tirzepatide: pause 7+ days before elective surgery
- For daily liraglutide: pause 24 hours before
- Treat emergency surgery on a GLP-1 patient as "full stomach"
A separate issue: bowel prep quality for colonoscopy is significantly worse on GLP-1s, leading to a notable increase in repeat colonoscopies.
NAION (Optic Nerve)
Detailed in the GLP-1 and blindness article. Observational data shows ~4× elevated NAION risk with semaglutide in some cohorts, no significant increase in others. Tirzepatide does not show the same signal.
Thyroid C-Cell Tumors (Boxed Warning)
Rats developed thyroid C-cell tumors in pre-clinical studies. Human data has not confirmed this signal, but the boxed warning remains. People with personal or family history of medullary thyroid carcinoma or MEN2 should not take any GLP-1.
Mental Health and Mood
Reports of suicidal ideation prompted FDA and EMA investigations. Trial data has not confirmed a causal link, but ongoing monitoring is part of standard checkup.
Worsening Diabetic Retinopathy
Rapid A1C drops can transiently worsen diabetic retinopathy. Patients with pre-existing retinopathy should have eye stabilization before rapid GLP-1 titration.
The "Tolerability Drift" Pattern
Most patients report side effects in a U-shape:
- Months 1–3: Peak side effects during titration
- Months 4–12: Mostly settle — the "honeymoon" period
- Year 2+: New issues may emerge — fatigue patterns, hair thinning (often from rapid weight loss, not the drug itself), face changes, plateaus, persistent mild constipation
This is partly drug effect, partly the downstream of being at a much lower body weight.
What Long-Term Monitoring Looks Like
A reasonable annual check on a stable GLP-1 patient:
| Test or check | Why |
|---|---|
| Weight and waist | Track plateau or rebound |
| Blood pressure | Confirm continued improvement |
| A1C and fasting glucose | If diabetic |
| Lipid panel | Track cardiovascular benefit |
| Liver enzymes | Track NAFLD/MASH improvement |
| Kidney function | Confirm safety, especially in CKD |
| TSH | Routine thyroid screening |
| Vitamin B12, vitamin D | Often low after sustained weight loss |
| Iron, ferritin | Especially in menstruating women |
| Body composition (DEXA or InBody) | If concerned about lean mass |
| DEXA bone density | Post-menopausal or other at-risk patients |
| Eye exam | Yearly if diabetic; consider baseline for NAION risk |
| Gallbladder ultrasound | If RUQ symptoms or rapid weight loss |
What Happens When People Stop
The cleanest long-term safety question: what happens after discontinuation?
- GI symptoms typically resolve within 4–8 weeks
- Weight regain in semaglutide withdrawal studies: patients regained about 2/3 of weight lost; net loss at 120 weeks was only 5.6%
- Lean mass loss does not automatically reverse — it has to be actively rebuilt
- Cardiometabolic gains partially reverse with weight regain
- Chronic gastroparesis in the rare patients who develop it can persist long after discontinuation
Stopping a GLP-1 abruptly is generally safe medically. The loss of appetite suppression often produces rebound hunger; tapering is increasingly common.
What People Get Wrong About Long-Term Use
- "I have to stop after a year — it's not safe forever." No clinical evidence supports a hard time limit. Many patients stay on indefinitely.
- "Side effects only get worse over time." Most actually fade. Long-term issues are different from the early ones.
- "I lost weight, so I can stop." Stopping usually leads to ~2/3 regain over time. Treat obesity like other chronic conditions.
- "It hasn't been studied long enough." Semaglutide has been on the market over a decade for diabetes. SELECT outcomes data extends to 5+ years.
Frequently Asked Questions
What are the long-term side effects of GLP-1 medications? Most side effects fade after 3–6 months. Longer-term concerns include lean muscle loss, bone density loss, gallbladder disease (2.6% on semaglutide vs 1.2% placebo), rare pancreatitis, persistent gastroparesis in a small subset, the semaglutide NAION signal, and anesthesia/procedure considerations.
Are GLP-1s safe long term? The 5+ year safety profile for semaglutide and shorter-term data for tirzepatide are reassuring. Monitoring is needed but the class is not currently considered high-risk for long-term use.
Do you have to stop a GLP-1 after a year? No. Obesity is a chronic condition, and most prescribers treat GLP-1s as long-term therapy when they are working.
Will I lose muscle on a GLP-1 long term? Yes, some — typically 25–40% of total weight lost can be lean mass without strength training. Resistance training and adequate protein significantly reduce this.
Do the GI side effects ever go away? For most patients, yes, within 3–6 months at stable dose. Some patients have persistent mild GI symptoms throughout treatment.
What happens to weight loss after I stop? Withdrawal studies of semaglutide showed patients regained about 2/3 of weight lost, with net loss of only 5.6% at 120 weeks.
How long should I stop before surgery? Withhold weekly GLP-1s (semaglutide, tirzepatide) for at least 7 days before elective surgery. Withhold daily GLP-1s (liraglutide, oral semaglutide, Foundayo) for 24 hours.
Last reviewed: May 13, 2026