


This is one of the most common questions in the entire GLP-1 conversation, and it comes up because the two drugs look similar on the surface. Ozempic comes in a pen. Insulin comes in a pen. Both are injected. Both are used in type 2 diabetes. Both have something to do with blood sugar. So the assumption — that semaglutide is "a new kind of insulin" or "insulin in a weekly shot" — is everywhere.
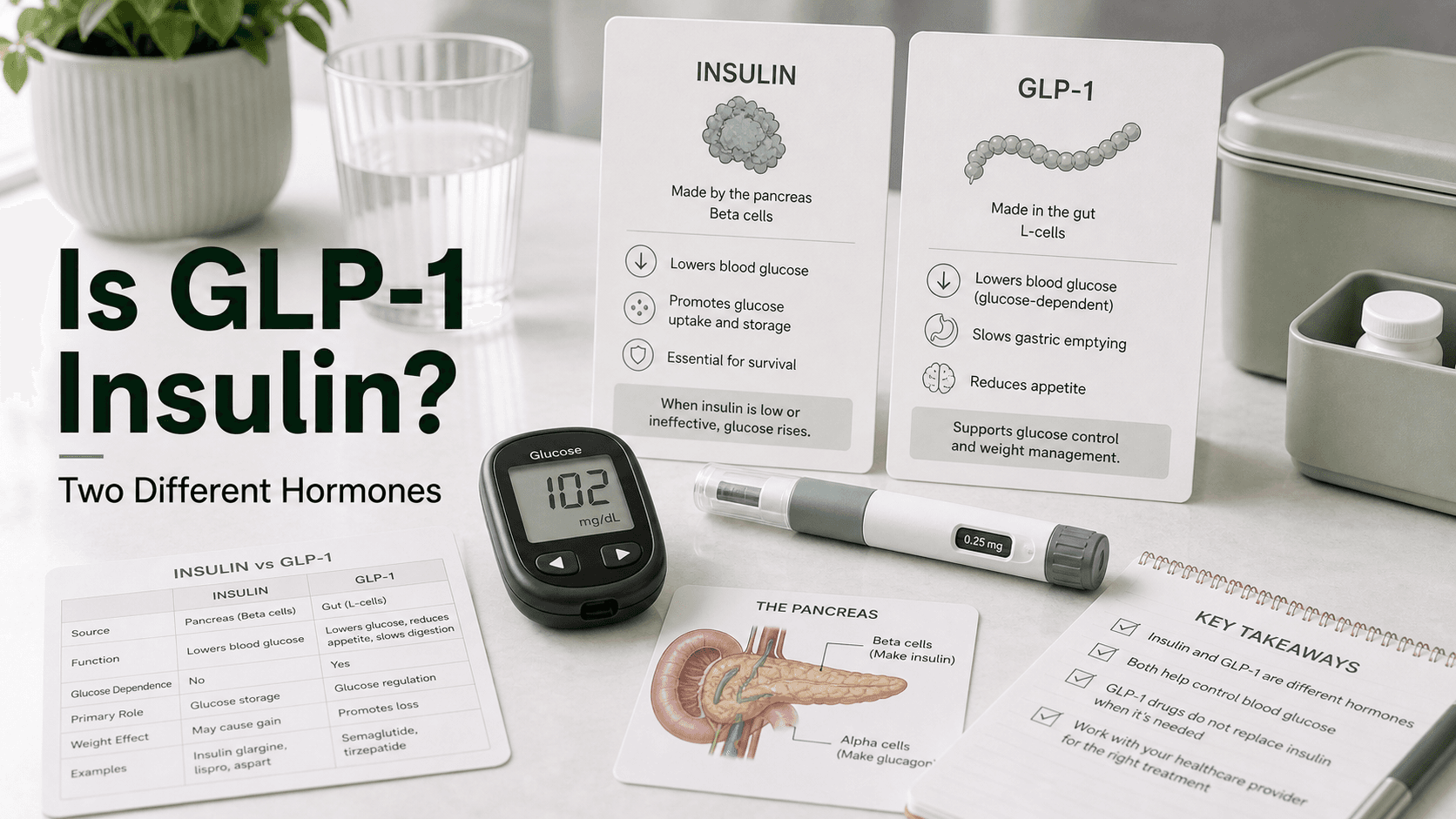
Direct answer: GLP-1 is not insulin. They are two different hormones with two different jobs. Insulin is a 51-amino-acid hormone made by pancreatic beta-cells; its single function is to lower blood glucose by pushing glucose into your cells. GLP-1 (glucagon-like peptide-1) is a 30-amino-acid incretin hormone made by intestinal L-cells; its job is to trigger the release of your own insulin after a meal, slow gastric emptying, suppress glucagon, and reduce appetite. Drugs like semaglutide (Ozempic, Wegovy, Rybelsus) and tirzepatide (Mounjaro, Zepbound) are GLP-1 receptor agonists — they mimic GLP-1, not insulin. Both classes are used in diabetes, often together, but the mechanisms, side effects, hypoglycemia risks, and price tags are very different.
What Insulin Actually Is
Insulin is a peptide hormone first isolated in 1921 and now the longest-running injectable diabetes therapy in medicine. The molecule has 51 amino acids arranged in two chains (A-chain of 21 and B-chain of 30) linked by disulfide bonds.
- Where it comes from: Pancreatic beta-cells in the islets of Langerhans
- Trigger for release: Rising blood glucose after a meal (and, secondarily, signals like GLP-1)
- Receptor: Insulin receptor (IR) — a tyrosine kinase receptor on essentially every cell in the body
- Effect: Tells muscle, fat, and liver cells to take glucose out of the bloodstream, store it as glycogen or fat, and stop making new glucose
Insulin's job is, simply, to lower blood glucose. That is the entire mechanism. It does not act on appetite, it does not act on gastric emptying, and it does not act on the gut. If your beta-cells stop making insulin (type 1 diabetes) or stop making enough of it (advanced type 2 diabetes), you need to inject it from outside, because no other drug fully replicates what insulin does.
Modern injectable insulins are bioengineered analogs of human insulin and come in three main flavors:
- Rapid-acting (lispro, aspart, glulisine) — taken at meals
- Long-acting / basal (glargine, detemir, degludec, icodec) — taken once daily or once weekly to cover background glucose
- Mixed / intermediate (NPH, premixed combinations)
The "type" only describes how fast the molecule is absorbed; the drug is the same hormone.
What GLP-1 Actually Is
GLP-1 is one of two incretin hormones — gut hormones released after eating that prime the pancreas to release insulin. The other incretin is GIP. Native GLP-1(7-36) amide is 30 amino acids long, with a plasma half-life of about 2 minutes before the DPP-4 enzyme breaks it down.
- Where it comes from: Intestinal L-cells (lower small intestine and colon), plus a small population of brainstem neurons
- Trigger for release: Food entering the gut — especially carbs and fats
- Receptor: GLP-1 receptor (GLP-1R) — a G-protein-coupled receptor found on pancreatic beta-cells, the stomach, the brainstem and hypothalamus, the heart, and the kidneys
- Effect: A whole bundle of things — listed below
Activating the GLP-1 receptor does not lower glucose directly. Instead, it sets off:
- Glucose-dependent insulin release from beta-cells — only when blood sugar is already high
- Suppressed glucagon secretion from alpha-cells — so the liver stops dumping glucose
- Slowed gastric emptying — the meal trickles into the bloodstream instead of spiking it
- Reduced appetite and "food noise" — via receptors in the hypothalamus
- Cardiovascular and renal benefits — shown in the SELECT and FLOW trials with semaglutide
GLP-1 receptor agonists — semaglutide, tirzepatide, liraglutide, dulaglutide, exenatide — are synthetic analogs of GLP-1, modified to resist DPP-4 cleavage so they last from hours to a week instead of two minutes. They are sometimes called "incretin mimetics." They are not insulin.
Side-By-Side
| Insulin | GLP-1 (and GLP-1 receptor agonists) | |
|---|---|---|
| Hormone class | Pancreatic peptide hormone | Incretin (gut peptide hormone) |
| Amino acid length | 51 (two chains) | 30 (GLP-1(7-36) amide) |
| Where produced | Pancreatic beta-cells | Intestinal L-cells, brainstem neurons |
| Receptor | Insulin receptor (everywhere) | GLP-1R (pancreas, brain, gut, heart, kidney) |
| Native half-life | 4–6 minutes | ~2 minutes |
| Primary action | Push glucose into cells (lowers blood sugar directly) | Trigger insulin release, slow gastric emptying, suppress appetite |
| Glucose-dependent? | No — lowers glucose whether high or low | Yes — only stimulates insulin when glucose is elevated |
| Hypoglycemia risk alone | Substantial | Very low |
| Appetite effect | Often increases appetite / weight gain | Suppresses appetite / weight loss |
| Approved for type 1 diabetes? | Yes — required | No (none of the GLP-1 drugs are first-line for T1D) |
| Approved for type 2 diabetes? | Yes | Yes |
| Approved for obesity? | No | Yes (semaglutide, tirzepatide, liraglutide) |
| Brand examples | Lantus, Tresiba, Humalog, NovoLog, Awiqli | Ozempic, Wegovy, Mounjaro, Zepbound, Trulicity, Victoza |
| Typical US monthly cost | $35 (with caps/programs) to $300+ | $25 (compounded) to $1,300 (Wegovy list) |
Where the Mechanisms Overlap — and Where They Do Not
The overlap is small and easy to misread. Both drugs end up lowering blood glucose, and both involve insulin in some way. But the how is different:
- Insulin is the hormone that lowers glucose. It binds receptors on muscle, fat, and liver cells and tells them to absorb glucose. No middleman.
- GLP-1 is the hormone that tells your body to release more insulin. It binds receptors on beta-cells and amplifies their natural response to a meal. It also does several non-insulin things — slowing the stomach, quieting appetite — that injectable insulin does not do.
A useful analogy: insulin is the worker that physically moves glucose into the warehouse. GLP-1 is the manager that calls the worker in when a delivery shows up. If the worker has been laid off — as in type 1 diabetes — calling the manager does not help. You need the worker back. That is why GLP-1 drugs do not replace insulin in type 1 diabetes.
When Each Is Prescribed
Insulin is prescribed when:
- A patient has type 1 diabetes — required for life, because the pancreas cannot make insulin
- A patient has late-stage type 2 diabetes where beta-cells have failed and oral or GLP-1 therapy can no longer keep A1c in range
- A patient has gestational diabetes that is not controlled by diet
- A patient is hospitalized with very high glucose levels and needs rapid correction
- A patient has type 2 diabetes with very high A1c at diagnosis (often a temporary use to stabilize blood sugar)
GLP-1 receptor agonists are prescribed when:
- A patient has type 2 diabetes and needs better glycemic control with weight loss
- A patient has obesity or overweight with weight-related conditions (semaglutide and tirzepatide are approved for chronic weight management)
- A patient with type 2 diabetes has cardiovascular or kidney disease — semaglutide and dulaglutide have outcome benefits
- A patient on insulin is gaining weight and the prescriber wants to add a GLP-1 to reduce insulin doses
GLP-1 drugs are not standalone therapy for type 1 diabetes. A few studies have tested them as add-ons to insulin in type 1, but they are not approved for it.
Can You Use Both Together?
Yes — and this is increasingly common in type 2 diabetes. The combination is supported by trials including SUSTAIN 5, which added semaglutide to basal insulin in patients with inadequately controlled type 2 diabetes:
- HbA1c reduction: 1.4% with semaglutide 0.5 mg and 1.8% with semaglutide 1.0 mg, versus 0.1% with placebo
- Body weight reduction: 3.7 kg and 6.4 kg respectively, versus 1.4 kg with placebo
- Total daily insulin dose: Reduced in the semaglutide groups
Newer combinations include tirzepatide added to insulin in advanced type 2 diabetes, and once-weekly insulin icodec plus semaglutide, which has performed comparably to traditional basal-bolus regimens in trials.
The clinical rationale: insulin handles the residual glucose-lowering need; GLP-1 reduces insulin requirements, controls post-meal spikes via slowed gastric emptying, and offsets the weight gain insulin tends to cause.
Important caveats:
- The two drugs should never be mixed in the same syringe.
- When a GLP-1 is added to insulin, the insulin dose is typically reduced by 20% or more to avoid hypoglycemia.
- The combination requires close glucose monitoring, especially during dose escalation.
Hypoglycemia Risk — The Single Biggest Practical Difference
This is the safety distinction that matters most in everyday use.
Insulin can drive blood sugar below normal — even dangerously low — on its own. It does not care what your glucose level is when you inject it; it will push glucose into cells regardless. Skip a meal, inject the same dose, and your blood sugar can crash. Hypoglycemia is the single most common adverse effect of insulin therapy and the main reason continuous glucose monitors became standard of care.
GLP-1 drugs essentially cannot cause hypoglycemia on their own, because they only stimulate insulin release when blood glucose is elevated. When your glucose is in the normal range, the beta-cells stop responding to GLP-1's signal. This is called glucose-dependent insulinotropic action and is the reason GLP-1s are considered relatively safe from a hypoglycemia standpoint.
The exceptions:
- GLP-1 + insulin combination: Hypoglycemia risk is now driven by the insulin, not the GLP-1. Dose adjustments are essential.
- GLP-1 + sulfonylurea (glipizide, glyburide): Sulfonylureas force insulin release regardless of glucose, so adding GLP-1 on top can cause lows.
- GLP-1 alone in a person with very tight glucose control can occasionally cause mild lows, but this is uncommon.
Cost — Same Class of Question, Very Different Numbers
Both are injectables, but pricing lives in different universes.
Insulin in the US in 2026:
- Standard out-of-pocket has settled near $35 per month for most patients due to Medicare caps, manufacturer cash programs (Eli Lilly, Novo Nordisk, Sanofi), and the Inflation Reduction Act
- Without programs, list prices for long-acting insulin pens can run $150–$500 per box
- Generic / biosimilar insulins (e.g., insulin aspart-szjj, insulin glargine-yfgn) have pushed prices down further
GLP-1 agonists in the US in 2026:
- Compounded semaglutide / tirzepatide (where still available): $99–$400 per month
- Branded telehealth cash pay (Wegovy, Zepbound through manufacturer direct programs): $199–$499 per month
- List price without insurance: $968–$1,349 per month for Ozempic, Wegovy, Mounjaro, Zepbound
- With commercial insurance and savings cards: as low as $25 per month for some patients with diabetes coverage
The headline number: insulin is currently 20–30x cheaper than branded GLP-1 therapy at full list price. That cost gap is shrinking but remains the main reason payers gate GLP-1 access more aggressively than insulin.
What People Get Wrong
- "Ozempic is just a new kind of insulin." It is not insulin at all. It is a GLP-1 receptor agonist. It binds a different receptor and does different things.
- "If insulin and GLP-1 both lower blood sugar, they must work the same way." Insulin lowers glucose by direct cellular uptake. GLP-1 lowers glucose mostly by triggering your own insulin release and slowing gastric emptying.
- "Type 1 diabetics can switch from insulin to Ozempic." No. Type 1 diabetes requires insulin. GLP-1 drugs do not replace it. Stopping insulin in a type 1 patient is medically dangerous and can cause diabetic ketoacidosis.
- "You cannot take insulin and a GLP-1 together." You absolutely can — it is a standard combination in type 2 diabetes. They just cannot be in the same syringe.
- "GLP-1 drugs cause hypoglycemia like insulin does." On their own, they rarely do. The hypoglycemia risk people worry about almost always comes from a co-prescribed insulin or sulfonylurea.
- "Both drugs cause weight gain." Insulin tends to cause weight gain. GLP-1 drugs cause weight loss. This is one reason combining them in type 2 diabetes is attractive.
Frequently Asked Questions
Is GLP-1 the same as insulin? No. GLP-1 is an incretin hormone (30 amino acids, made in the gut) that triggers insulin release. Insulin is the hormone (51 amino acids, made in the pancreas) that actually moves glucose into cells. Different molecules, different receptors, different jobs.
Is Ozempic insulin? No. Ozempic is semaglutide, a GLP-1 receptor agonist. It mimics the gut hormone GLP-1, not insulin. It does, however, increase your body's own insulin output in response to meals.
Does Ozempic contain insulin? No. There is no insulin in Ozempic, Wegovy, Mounjaro, Zepbound, Trulicity, or Victoza. The active ingredient in each is a GLP-1 (or dual GLP-1/GIP) agonist peptide.
Can a type 1 diabetic stop insulin and take a GLP-1 instead? No. Type 1 diabetics produce no insulin and require external insulin to survive. GLP-1 drugs do not replace insulin and are not approved for type 1 diabetes.
Can you take Ozempic and insulin at the same time? Yes, this is a common combination in type 2 diabetes. They must be given in separate injections (not the same syringe) and insulin doses are usually lowered to reduce hypoglycemia risk.
Which causes hypoglycemia, insulin or GLP-1? Insulin can cause hypoglycemia on its own. GLP-1 drugs almost never cause hypoglycemia on their own because they only stimulate insulin release when glucose is high. The risk rises when GLP-1s are combined with insulin or sulfonylureas.
Is GLP-1 cheaper than insulin? No, generally the opposite. In the US, insulin is currently around $35 per month for most patients thanks to caps and manufacturer programs. Branded GLP-1 therapy ranges from $25 (with coverage) to $1,300+ per month at list price.
Why do people confuse GLP-1 with insulin? Both are injectable peptide hormones, both are used in type 2 diabetes, both come in pens, and both affect blood sugar. The everyday similarities are large; the molecular biology is not.
Last reviewed: May 13, 2026
Sources
- Glucagon-like peptide-1 — Wikipedia
- GLP-1 receptor activated insulin secretion from pancreatic beta-cells: mechanism and glucose dependence — PMC
- GIP and GLP-1, the two incretin hormones: Similarities and differences — PMC
- GLP-1 Agonists: What They Are, How They Work and Side Effects — Cleveland Clinic
- Is Ozempic Insulin? Key Differences Explained — Ro
- Is Ozempic the Same as Insulin? — Dr. Shima Hadidchi MD
- Does Ozempic replace insulin? — SingleCare
- Semaglutide Added to Basal Insulin in Type 2 Diabetes (SUSTAIN 5) — PMC
- Transitioning From MDI Insulin to Semaglutide — Cleveland Clinic Consult QD
- Glucagon-like peptide-1 receptor: mechanisms and advances in therapy — Nature, Signal Transduction and Targeted Therapy
- Combination insulin icodec and semaglutide cuts HbA1c and body weight in type 2 diabetes — Healio




