The average participant on tirzepatide 15mg lost 22.5% of their body weight over 72 weeks — a number that rivals bariatric surgery and rewrites what a medication can do for obesity.
SURMOUNT-1, 15mg dose
Primary endpoint
On 15mg, ~231 lb baseline
Key Takeaways
- Tirzepatide produced 16–22.5% body weight loss depending on dose in SURMOUNT-1 — roughly 3–4× what older weight loss drugs achieved
- SURMOUNT-2 confirmed similar results in people with type 2 diabetes, though losses were slightly lower (~15.7% at 15mg)
- Most of the weight lost is fat, not muscle — body composition data shows roughly 70% fat mass reduction vs 30% lean tissue
- Real-world results tend to run 10–20% lower than trial averages due to less controlled conditions and adherence variation
- Weight loss slows or plateaus around month 6–9 for most people; this is expected, not failure
- Higher starting BMI, better adherence, and combining tirzepatide with diet changes predict the strongest outcomes
The clinical data on tirzepatide is genuinely impressive — not hype, not extrapolation, but Phase 3 trial numbers from over 10,000 participants. What those numbers don't show is the month-by-month experience: the slow first few weeks, the inflection point where appetite suddenly shifts, or the plateau that catches people off guard around month seven.
This guide walks through both: what the trials proved, and what actually happens when real people use tirzepatide over months and years. If you're evaluating whether tirzepatide is worth it, this is the data you need.
What SURMOUNT-1 Actually Showed
SURMOUNT-1 is the foundational trial for tirzepatide and weight loss. Published in the New England Journal of Medicine in 2022, it enrolled 2,539 adults with obesity (BMI ≥30) or overweight (BMI ≥27 with at least one weight-related comorbidity) but without type 2 diabetes. Participants received once-weekly subcutaneous injections of tirzepatide at 5mg, 10mg, or 15mg — or placebo — for 72 weeks (about 17 months).
The primary endpoint was percentage change in body weight from baseline. All three doses beat placebo decisively. The headline numbers:
| Dose | Avg Weight Loss % | Avg Absolute Loss | ≥5% threshold | ≥20% threshold |
|---|---|---|---|---|
| 5mg | 16.0% | ~35 lbs | 89% | 39% |
| 10mg | 21.4% | ~49 lbs | 96% | 57% |
| 15mg | 22.5% | ~52 lbs | 96% | 63% |
| Placebo | 2.4% | ~5 lbs | 28% | 3% |
The difference between 10mg and 15mg is narrower than you'd expect — less than a percentage point. That's not a measurement error; it suggests the 10mg dose is close to the dose-response ceiling for most people. The jump from 5mg to 10mg is where the biggest gain happens.
What makes SURMOUNT-1 results particularly striking is the threshold data. For 10mg and 15mg users, 78–84% lost at least 10% of their body weight. Between 67–71% lost at least 15%. And 50–57% lost 20% or more. These figures had previously been seen only with bariatric surgery.
How Tirzepatide Works: Dual GIP/GLP-1 Agonism
Tirzepatide is a dual agonist: it activates both the GIP receptor and the GLP-1 receptor, unlike single-agonist GLP-1 drugs such as semaglutide that target the GLP-1 receptor alone. The drug's label states that tirzepatide increases insulin sensitivity, enhances insulin secretion, and delays gastric emptying, and the added GIP receptor activity is the leading hypothesis for why tirzepatide tends to produce more weight loss than GLP-1-only medications. GLP-1 receptor activation is the pathway driving much of the appetite suppression and slowed gastric emptying described in the month-by-month timeline below.
SURMOUNT-2: Results in People with Type 2 Diabetes
SURMOUNT-2 answered a separate question: how well does tirzepatide work for weight loss in people who already have type 2 diabetes? This matters because diabetes itself — and many diabetes medications — can make weight loss harder.
SURMOUNT-2 enrolled 938 adults with T2D and a BMI ≥27. The same doses (5mg, 10mg, 15mg) were tested over 72 weeks. Results were strong, but modestly lower than SURMOUNT-1:
- 5mg: ~13.9% body weight loss
- 10mg: ~15.4%
- 15mg: ~15.7%
The gap vs SURMOUNT-1 is about 6–7 percentage points at the high end. That's meaningful but not disqualifying — a 15.7% reduction in someone weighing 240 lbs is still roughly 37 lbs lost. Blood sugar control also improved dramatically: HbA1c dropped by 1.6–2.1 percentage points across doses, and many participants were able to reduce or discontinue other diabetes medications.
For people navigating both obesity and T2D, this is particularly relevant: tirzepatide addresses both conditions simultaneously. Read more about tirzepatide for weight loss for a deeper breakdown of how it works across different metabolic profiles.
Tirzepatide Weight Loss by Dose: The Real Tradeoffs
Not everyone ends up on 15mg. The tirzepatide dosage protocol starts at 2.5mg for the first four weeks and escalates by 2.5mg every four weeks until the target dose is reached. Many people can't tolerate the higher doses without persistent nausea; others plateau early and benefit from pushing higher.
Here's how the dose decision tends to play out in practice:
5mg — Often used as a maintenance dose by people who reached their goal weight and want to hold it. Also the ceiling for some individuals with GI sensitivity. Delivers real results, but the gap vs 10mg is significant enough that most providers aim higher.
10mg — The sweet spot for many people. Strong results, typically manageable side effects, and the evidence base from SURMOUNT-1 is compelling. The difference between 10mg and 15mg in absolute weight loss is roughly 3 lbs on average — not dramatic.
15mg — The maximum approved dose. Where the ceiling of tirzepatide's effect lives. Best results in trials, but also the most nausea and GI side effects during the dose escalation phase.
If you're deciding where to land on the dosing ladder, look at your goal, your tolerance, and how your appetite responds as you escalate. Some people get dramatic results at 5mg; others need 15mg to see real movement.
Note that 7.5mg is a real step on the ladder, not just a number you pass through. Per the approved dosing schedule, the titration runs 2.5mg, 5mg, 7.5mg, 10mg, 12.5mg, and 15mg, so 7.5mg often serves as an intermediate maintenance dose for people who get good results before reaching the top of the range or who need a slower escalation for tolerability.
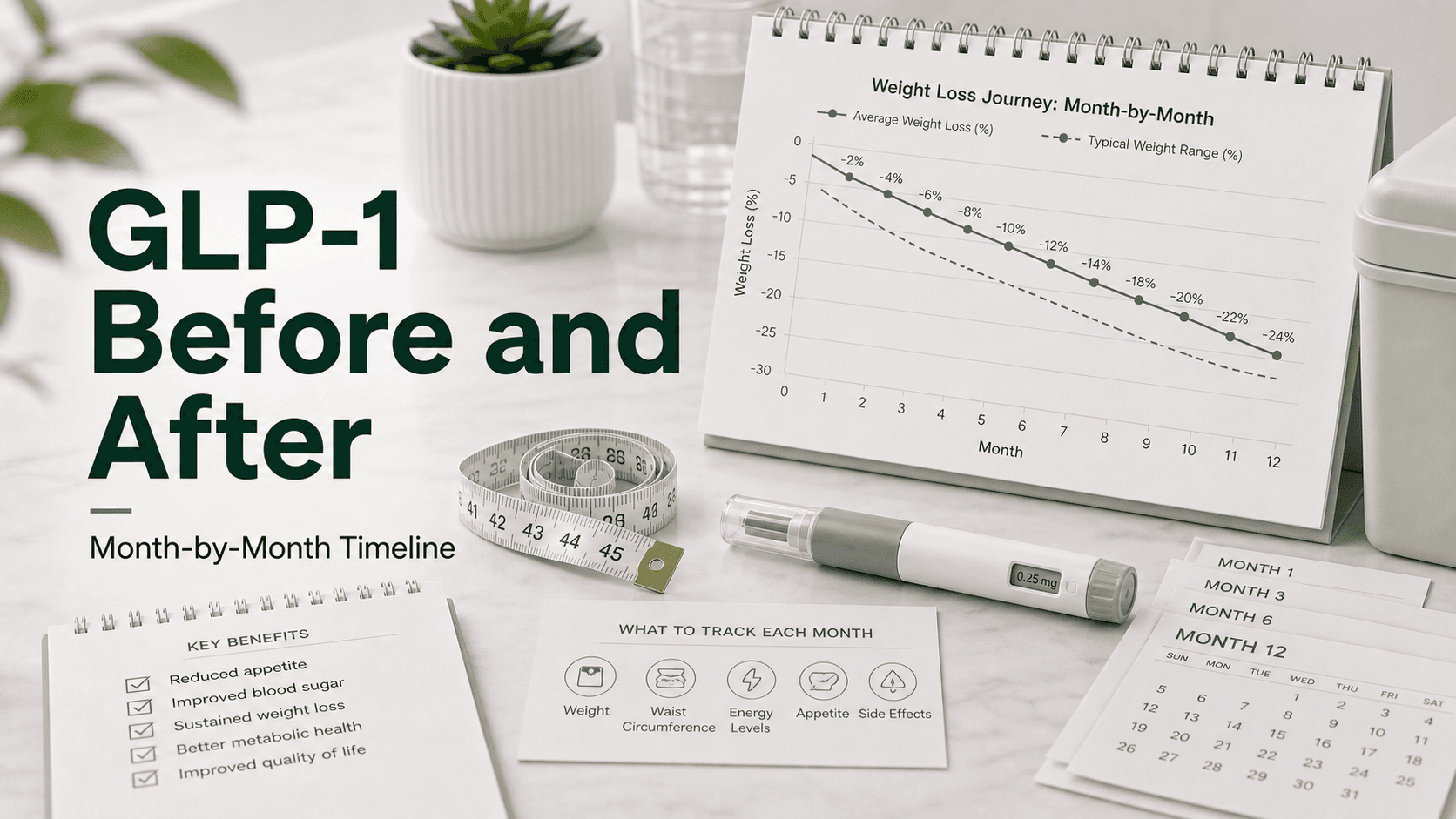
Tirzepatide Before and After: Month-by-Month Timeline
This is what a typical tirzepatide journey looks like based on trial data and real-world patterns. Individual variation is wide, but the general shape holds.
| Timeframe | Typical Weight Loss | What's Happening |
|---|---|---|
| Weeks 1–4 | 2–5 lbs | Appetite suppression begins. Many feel it within 1–2 weeks. Nausea is common on dose escalation days. Scale moves slowly. |
| Months 1–3 | 8–15 lbs | Loss accelerates as dose escalates. Energy often improves. GI side effects typically improve after the first escalation. |
| Months 3–6 | 15–30 lbs total | The fastest phase for most people. Appetite at its most suppressed. Physical changes become noticeable to others. |
| Months 6–9 | Rate slows | The natural plateau window. Loss doesn't stop, but weekly rate drops significantly. Patience matters here. |
| Months 9–18 | Continued loss or maintenance | Progress continues but slower. Some people reach their goal weight; others are still losing. Body composition changes continue even when scale slows. |
One thing that surprises people: the first month isn't always dramatic. You're on 2.5mg, which is more of a tolerance-building dose than a full therapeutic one. Some people see immediate, significant loss; others don't notice the scale move until weeks 6–8 when they've reached the 5–7.5mg range. Don't write it off in month one.
Side Effects During the Before-and-After Journey
The most common side effects are gastrointestinal, and they tend to cluster around the dose-escalation weeks. According to the drug label, the most common adverse reactions include nausea, diarrhea, decreased appetite, vomiting, and constipation. For most people these effects are most pronounced right after a dose step-up and ease over the following weeks, but persistent or severe symptoms are worth raising with your care team.
Body Composition: What You're Actually Losing
Weight loss numbers only tell part of the story. What matters as much as the scale is what you're losing — fat versus lean mass (muscle, bone, water).
The SURMOUNT-1 body composition sub-analysis showed that roughly 70% of the weight lost was fat mass, with the remaining 30% coming from lean mass (including muscle). That ratio is roughly in line with what you'd see from diet-only weight loss, but there's nuance here.
The concern with any rapid weight loss intervention is muscle loss. Lean mass loss of 30% of total weight lost sounds significant — and it is worth monitoring. However, in absolute terms, people who lost 52 lbs on 15mg lost roughly 36 lbs of fat and 16 lbs of lean tissue. Maintaining or building lean mass while on tirzepatide is possible and worth actively pursuing through resistance training and adequate protein intake.
What improved alongside body composition:
- Waist circumference: average reduction of 6–7 cm
- Visceral fat (the dangerous abdominal variety): significant reduction
- Blood pressure, triglycerides, and HbA1c all improved substantially
- HDL cholesterol increased; LDL effects were more variable
The "after" picture of tirzepatide isn't just a lower number on a scale — it's a different metabolic profile.
Beyond the fat-versus-lean breakdown, the metabolic "after" picture includes better insulin handling: the drug label notes that tirzepatide increases insulin sensitivity and enhances insulin secretion, which helps explain the HbA1c reductions seen in the SURMOUNT-2 population above.
Real-World Results vs Trial Data: The Gap You Should Expect
Clinical trials are controlled environments. Participants are monitored closely, medication is provided free, and adherence is tracked carefully. That's not how it works in the real world.
Real-world data consistently shows results running 10–20% below trial averages. The main reasons:
Adherence gaps. Skipping doses, pausing due to supply issues, or stopping when GI symptoms get rough all blunt results.
Dose ceiling. Many real-world patients never reach 15mg. Insurance coverage, cost, or side effects push people to stay at 5–10mg.
Diet and lifestyle. Trial participants received nutrition counseling. Most people using tirzepatide outside a trial don't have structured dietary support.
Selection effects. Trials exclude people with certain conditions. Real-world users have more variability.
A reasonable expectation outside of a trial: 10–18% body weight loss over 12–18 months if you're consistent, escalate your dose appropriately, and make some lifestyle adjustments. That's still transformative for most people — but setting a realistic target matters.
The Plateau: Why It Happens and What to Do
Around months 6–9, the rate of loss slows for nearly everyone on tirzepatide. This isn't a failure of the drug — it's a biological response called adaptive thermogenesis. As body weight drops, your resting metabolic rate decreases, and your body becomes more efficient at maintaining its new lower weight.
Tirzepatide continues to suppress appetite through the plateau, which is why weight doesn't typically regain during this phase (unlike most diet-based approaches). But the weekly loss that felt automatic in months 3–6 becomes more effort-dependent.
What actually helps during a tirzepatide plateau:
- Resistance training to preserve and build lean mass, which supports metabolic rate
- Reviewing protein intake — most people benefit from higher protein when losing weight
- Confirming you're at your maximum tolerated dose
- Not interpreting the slowdown as a reason to stop
What doesn't help: expecting the month-3 loss rate to continue indefinitely. It won't. That's true for every effective weight loss intervention, tirzepatide included.
Who Gets the Best Results on Tirzepatide
Not everyone responds equally. Several factors consistently predict stronger outcomes:
Higher starting BMI. People with more to lose tend to lose a higher absolute amount. The percentage loss is similar, but someone starting at 300 lbs will lose more lbs than someone starting at 220 lbs.
No type 2 diabetes. As SURMOUNT-1 vs SURMOUNT-2 showed, T2D is associated with lower weight loss response. Not disqualifying, but a realistic modifier.
Dose escalation to 10mg or above. The evidence strongly supports higher doses. If you're staying at 5mg for tolerability reasons, expect results closer to the lower end of the range.
Active lifestyle adjustments. Participants in SURMOUNT trials who paired tirzepatide with diet and movement saw better outcomes. The drug suppresses appetite; what you do with that appetite suppression matters.
Consistent, uninterrupted dosing. Supply disruptions and self-imposed breaks significantly reduce effectiveness. The drug's mechanism requires sustained activation to maintain its full effect.
People who tend to see more modest results: those with significant thyroid conditions, certain medications that interfere with GLP-1 signaling, very low starting BMIs, or who can't tolerate doses above 5mg.
Tirzepatide vs Retatrutide: The Next Frontier
Tirzepatide's results were already rewriting expectations — then retatrutide data emerged. Where tirzepatide is a dual agonist (GIP + GLP-1), retatrutide is a triple agonist (GIP + GLP-1 + glucagon receptors), and early Phase 2 data suggests it pushes the ceiling even higher.
Phase 2 retatrutide trial data (24 weeks, not 72) showed weight loss of approximately 17.5% on the highest dose. Extrapolated to 72 weeks, projections suggest 24–26% body weight loss — which would exceed tirzepatide's best documented results.
What this means in practice:
- Tirzepatide is still the gold standard with the strongest long-term evidence base
- Retatrutide is earlier in development with less safety/long-term data
- The addition of glucagon receptor agonism appears to drive greater fat oxidation and may be responsible for the additional weight loss
- For people who plateau on tirzepatide or are seeking the most aggressive pharmaceutical approach, retatrutide is worth watching
For a direct head-to-head on results, timelines, and mechanisms, see retatrutide before and after.
Mounjaro and Zepbound: Same Molecule, Different Labels
If you're seeing "Mounjaro before and after" or "Zepbound before and after" in your research, they're the same drug — tirzepatide. Eli Lilly developed tirzepatide as Mounjaro for type 2 diabetes management (FDA-approved May 2022), then re-submitted the same molecule as Zepbound for chronic weight management (FDA-approved November 2023).
The injection formulations are identical. The dosing options are the same. The only practical difference is the branded indication — Mounjaro is technically prescribed for T2D, Zepbound for obesity/overweight. Insurance coverage and copay cards differ between the two.
All the SURMOUNT trial data applies equally to both brand names. When you read "Mounjaro before and after" accounts online, those are tirzepatide results.
Ready to Start? What to Know First
If you're evaluating tirzepatide based on the evidence above, the results are compelling enough to warrant a serious conversation with a healthcare provider. Key things to confirm before starting:
- You meet criteria: BMI ≥30, or BMI ≥27 with a weight-related condition like hypertension, sleep apnea, or dyslipidemia
- You understand the escalation timeline: it takes 12–20 weeks to reach full dose
- You have a plan for managing GI side effects during dose escalation (eating smaller meals, avoiding high-fat foods)
- You're not using this as a quick fix — the data strongly suggests weight regain when tirzepatide is stopped without lifestyle changes in place
For supply options and pricing, Ascension Peptides carries tirzepatide with transparent sourcing and dosing support.
Frequently Asked Questions
How much weight can you lose on tirzepatide in 3 months? Most people lose 8–15 lbs in the first three months. The range is wide because you're still escalating your dose during this window, and individual response varies. People starting at higher weights tend to lose more in absolute terms early on.
What do tirzepatide before and after results look like at 6 months? At six months, most people who've tolerated dose escalation to 10mg or 15mg have lost 15–25 lbs or more. Body composition changes are visible — particularly in waist circumference and facial changes. This is typically when the physical transformation becomes obvious to others.
Is 22.5% weight loss realistic for everyone? No. That's the average for the 15mg group in SURMOUNT-1 — a highly controlled trial with perfect adherence and regular monitoring. Real-world results average 10–20% lower. Setting a goal of 15% body weight loss is more realistic for most people.
Does tirzepatide work the same for Mounjaro and Zepbound? Yes. Both Mounjaro and Zepbound are tirzepatide — same molecule, same dosing options, same mechanism. The brand name reflects the approved indication, not any difference in the drug itself.
What happens when you stop tirzepatide? The SURMOUNT-J extension study (and observational data) shows that weight regain is common after stopping, particularly without lifestyle behavior changes. Most participants regained roughly 50–66% of their lost weight within a year of discontinuation. This suggests tirzepatide is most effective as a long-term tool, not a short-term course.
How does tirzepatide before and after compare to semaglutide? Head-to-head in SURMOUNT-5, tirzepatide achieved 20.2% weight loss vs 13.7% for semaglutide at 72 weeks — about 6.5 percentage points more. This translates to roughly 15 additional pounds lost on average. Both are effective; tirzepatide consistently outperforms in direct comparisons.
When does tirzepatide start working? Appetite suppression typically starts within the first 1–2 weeks, even at the lowest 2.5mg starting dose. Scale changes usually lag by 2–4 weeks. Significant weight loss — enough to be visible in photos — typically takes 3–4 months.
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Tirzepatide is a prescription medication and should only be used under the supervision of a qualified healthcare provider. Individual results vary. Always consult your physician before starting, stopping, or changing any medication regimen.
Is semaglutide the same as Wegovy and Ozempic? Semaglutide, the comparator in SURMOUNT-5, is the active ingredient sold as Wegovy for chronic weight management and as Ozempic for type 2 diabetes, paralleling the Zepbound and Mounjaro framing used for tirzepatide. So "Wegovy before and after" results are semaglutide results, just as "Zepbound before and after" results are tirzepatide results.