GLP-1 medications slow gastric emptying. That is the entire reason anesthesiologists care about them before a procedure: a stomach that should be empty after overnight fasting may still contain food, and food in the stomach during sedation or general anesthesia can be regurgitated and aspirated into the lungs. The American Society of Anesthesiologists (ASA) issued its first formal guidance in June 2023, then joined four other societies in a revised multisociety statement in October 2024 that walked back the blanket "stop everyone" position in favor of risk-stratified, individualized decisions.
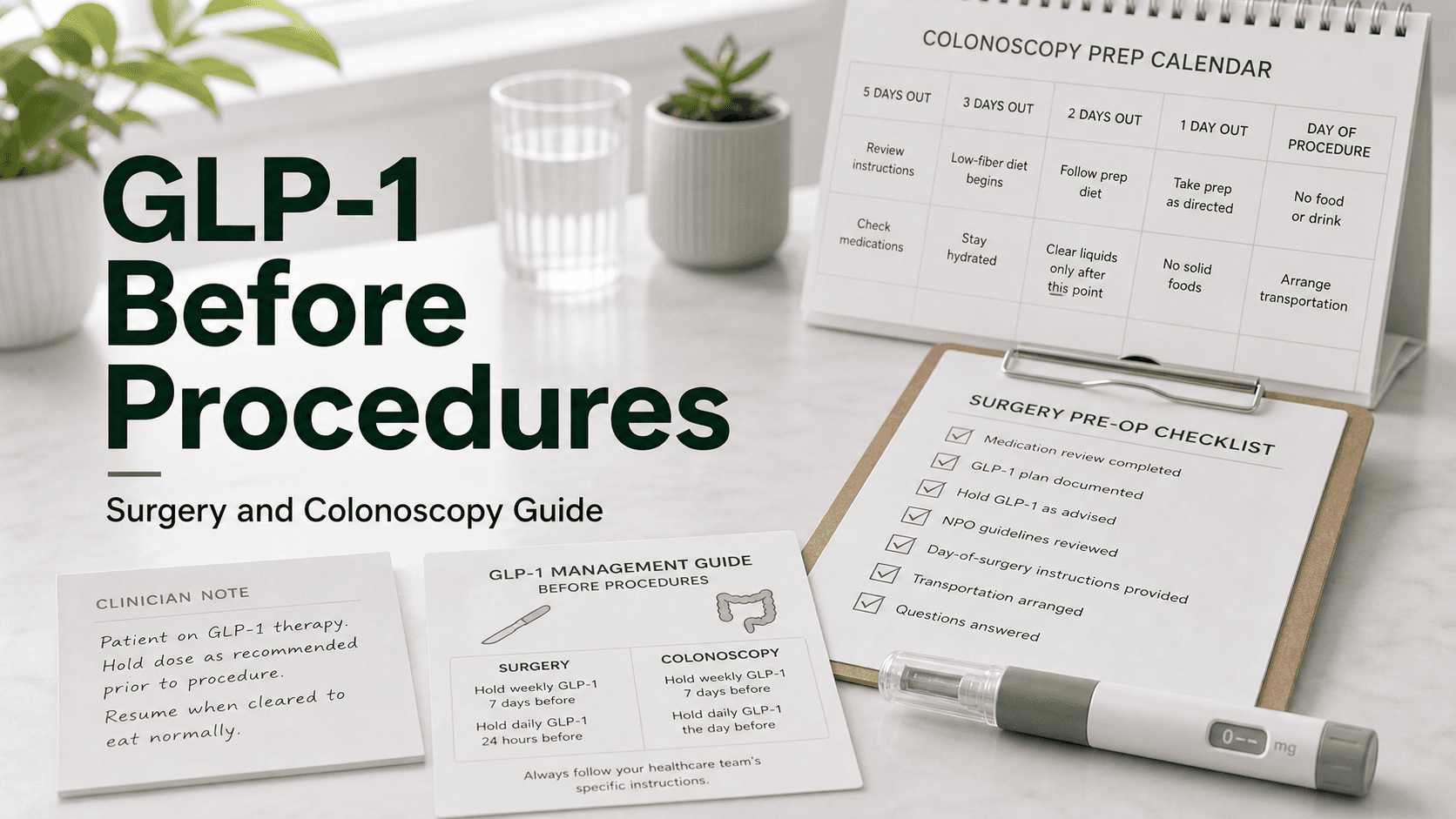
Direct answer: If your team follows the original ASA 2023 protocol, hold weekly GLP-1s (semaglutide, tirzepatide, dulaglutide) for 7 days before the procedure, and daily GLP-1s (liraglutide, oral semaglutide, lixisenatide) for 24 hours (skip the morning dose on procedure day). Under the 2024 multisociety update (ASA + AGA + ASMBS + ISPCOP + SAGES), most patients can continue their GLP-1 and follow a 24-hour clear liquid diet the day before the procedure instead — with holds reserved for higher-risk patients (dose escalation, GI symptoms, gastroparesis, max doses). Always tell your anesthesia team you take a GLP-1. For emergency surgery, the team should assume a "full stomach" and use rapid sequence intubation (RSI).
Why GLP-1s Matter Before Anesthesia
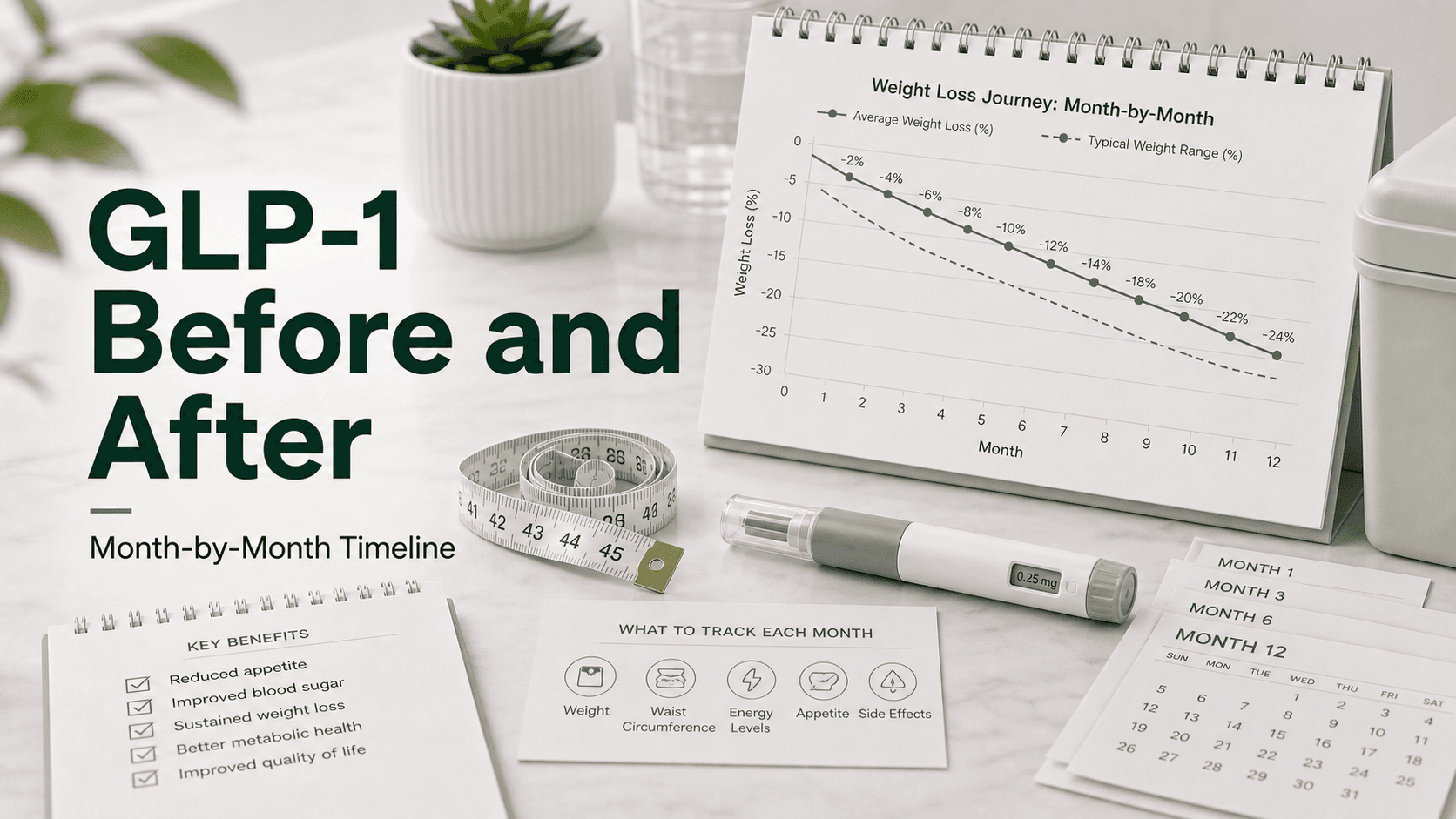
GLP-1 receptor agonists (semaglutide/Ozempic/Wegovy, tirzepatide/Mounjaro/Zepbound, liraglutide/Saxenda/Victoza, dulaglutide/Trulicity) work in part by slowing gastric emptying — solid food sits in the stomach about 36 minutes longer on average, with one study showing 72% retention at 2 hours and 37% retention at 4 hours. That same delay is what helps with satiety and post-meal glucose control. It is also the safety issue.
Under general anesthesia or deep sedation, protective airway reflexes are blunted. If gastric contents come back up the esophagus, they can be inhaled into the lungs — pulmonary aspiration. Aspiration of acidic stomach contents causes chemical pneumonitis; aspiration of solid food can obstruct the airway outright. Case reports in 2023 and 2024 documented patients on semaglutide who had full stomachs despite overnight fasting, including some who aspirated and required ICU care.
Two important caveats keep the actual risk in perspective:
- Tachyphylaxis. The gastric-slowing effect attenuates with continuous exposure — patients on stable maintenance doses for months have less delay than patients in dose escalation.
- Observational data. Large analyses have not shown a statistically significant increase in clinical aspiration rates in elective surgery among GLP-1 users versus non-users. The concern is real but the absolute risk is small.
The 2023 ASA Guidance (Still Used Many Places)
In June 2023 the ASA issued consensus-based (not evidence-based) guidance for the day before and day of elective surgery in adults and children on GLP-1 receptor agonists:
- Daily-dosed GLP-1s — hold the dose on the day of the procedure.
- Weekly-dosed GLP-1s — hold the dose for one week before the procedure.
- If GI symptoms (nausea, vomiting, abdominal distension, dyspepsia) are present on procedure day, consider delaying the procedure or treating as a full stomach.
- If the drug was not held and the patient is asymptomatic, consider gastric ultrasound to estimate residual contents.
- If retained contents are confirmed or suspected and the procedure must proceed, use rapid sequence intubation with cricoid pressure.
The one-week interval for weekly drugs reflects the ~5-7 day half-life of semaglutide and tirzepatide. Pharmacokinetically, one half-life still leaves substantial drug on board, and the ASA's choice was a practical compromise rather than a number derived from a randomized trial. Some 2024-2025 studies argued 10-14 days would be more reliable to clear residual gastric contents; one orthopedic study suggested 14 days for total joint arthroplasty.
The 2024 Multisociety Revision
In October 2024 a joint statement from five societies — the ASA, American Gastroenterological Association (AGA), American Society for Metabolic and Bariatric Surgery (ASMBS), International Society of Perioperative Care of Patients with Obesity (ISPCOP), and Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) — softened the approach.
Key shifts:
- Most patients can continue their GLP-1 before elective procedures.
- Shared decision-making between the patient, prescribing clinician, anesthesia team, and proceduralist replaces blanket rules.
- Higher-risk patients still warrant a hold or other mitigation:
- Dose-escalation phase (early in treatment or dose increase within last several weeks)
- Maximum doses (e.g., semaglutide 2.4 mg, tirzepatide 15 mg)
- Active GI symptoms (nausea, vomiting, bloating, reflux)
- Comorbidities affecting gastric motility (gastroparesis, Parkinson disease, scleroderma)
- Clear liquid diet for 24 hours before the procedure is the headline mitigation — modeled on bariatric and colonoscopy prep practice.
- Point-of-care gastric ultrasound the morning of the procedure can confirm an empty stomach if available.
- If the hold was missed and there are no symptoms, the procedure can usually proceed with standard precautions.
- If retained contents are suspected, options are RSI or rescheduling.
When a hold is decided under the 2024 guidance, the intervals are still daily on day of surgery, weekly one week prior — same numbers, but applied selectively.
Exact Stopping Intervals by Drug
| Drug | Brand | Frequency | ASA 2023 hold | 2024 update |
|---|---|---|---|---|
| Semaglutide injection | Ozempic, Wegovy | Weekly | 7 days | 7 days if held; otherwise 24-hr clear liquids |
| Tirzepatide | Mounjaro, Zepbound | Weekly | 7 days | 7 days if held; otherwise 24-hr clear liquids |
| Dulaglutide | Trulicity | Weekly | 7 days | 7 days if held; otherwise 24-hr clear liquids |
| Exenatide ER | Bydureon | Weekly | 7 days (long half-life — many hold 14 days) | Risk-based |
| Liraglutide | Saxenda, Victoza | Daily | Hold day of surgery | Often continued |
| Oral semaglutide | Rybelsus | Daily | Hold day of surgery | Often continued |
| Lixisenatide | Adlyxin | Daily | Hold day of surgery | Often continued |
| Exenatide IR | Byetta | Twice daily | Hold day of surgery | Often continued |
The pattern: weekly drugs have long half-lives and need long holds if held at all; daily drugs clear quickly and a one-day skip is enough.
Colonoscopy-Specific Guidance
Colonoscopy is the place where GLP-1s matter most for two reasons: bowel prep quality and sedation depth.
Bowel prep concerns. Delayed gastric emptying can compound with a large-volume polyethylene glycol prep, increasing nausea and vomiting during prep and making it harder to finish. Studies looking at adequacy of bowel prep in GLP-1 users found higher rates of inadequate prep in some series, though others found no difference once an extended liquid diet was used.
AGA position. The AGA was the most vocal society in pushing back against universal holds. Its stance, reflected in the 2024 multisociety guidance:
- Do not stop GLP-1s in everyone before elective endoscopy or colonoscopy.
- Proceed with the scheduled procedure if the patient followed standard fasting (8 hours solids, 2 hours clear liquids) and has no GI symptoms.
- Extended clear liquid diet (24 hours before the procedure) is the preferred mitigation rather than stopping the drug.
- If retained gastric contents are suspected and the procedure must proceed, consider rapid-sequence intubation — though that is generally not practical in outpatient endoscopy and usually means rescheduling.
For colonoscopy with deep sedation (propofol), the aspiration concern is real but lower than for full general anesthesia with intubation. Most endoscopy centers now combine the 24-hour clear liquid approach with intra-procedure airway vigilance.
Emergency Surgery
If you need urgent or emergency surgery and have not held your GLP-1, the anesthesia team should treat you as a "full stomach" regardless of when you last ate. That means:
- Rapid sequence intubation (RSI) with cricoid pressure to secure the airway quickly.
- Avoiding deep sedation without a protected airway when possible.
- Gastric decompression with a nasogastric tube if indicated.
- Antiemetic premedication to reduce vomiting.
- Gastric ultrasound if available and time permits to confirm or refute retained contents.
Do not lie about or omit your GLP-1 use because surgery is urgent. The team's plan changes with that information, and the change protects you.
Restart Timing After the Procedure
There is no single published rule for restarting, but practice is consistent:
- Minor procedures (outpatient endoscopy, small skin surgery): resume the GLP-1 within a few days — often the next scheduled weekly dose — at the previous dose once you are eating and not nauseated.
- Major abdominal or bariatric surgery: wait 1-2 weeks, until you tolerate oral intake without vomiting and your surgical team approves.
- If you were off less than 2 weeks total: resume at your previous dose.
- If you were off more than 2 weeks (or more than 4 weeks for some prescribers): restart at the lowest dose (e.g., semaglutide 0.25 mg, tirzepatide 2.5 mg) and re-titrate, because tolerance to GI side effects fades.
Starting too soon can stack post-op nausea on top of GLP-1 nausea, blunt appetite when you need calories for healing, and contribute to dehydration. Holding too long lets blood sugar climb in diabetic patients and rebound hunger return in weight-loss patients.
What to Tell Your Anesthesia Team
Before any procedure with sedation or anesthesia, tell them:
- The exact drug you take (semaglutide vs tirzepatide vs liraglutide — they are not interchangeable).
- The dose and how long you have been on it.
- The date of your last injection (or last oral dose).
- Whether you are in dose escalation or stable maintenance.
- Whether you have GI symptoms in the past 24-72 hours (nausea, vomiting, reflux, bloating, fullness).
- The indication — diabetes changes the conversation about holding because hyperglycemia is its own surgical risk.
A short, written list beats trying to remember at pre-op. If your prescribing clinician and your anesthesiologist disagree about whether to hold, ask them to talk directly.
Diabetes Management When Stopping
If you take a GLP-1 for type 2 diabetes, holding for a week can let blood glucose rise — and elevated perioperative glucose is associated with worse outcomes (infection, delayed wound healing). Strategies:
- Continue other diabetes medications unless told otherwise (metformin is usually continued; SGLT2 inhibitors are usually held).
- More frequent glucose checks during the hold period.
- Short-acting insulin coverage may be added by your endocrinologist or PCP.
- Avoid prolonged carb loading during the clear-liquid day, which can spike glucose.
- Have a plan before procedure day, not on procedure day.
For weight-loss-only GLP-1 users, holding a week typically means a small amount of weight regain and the return of food noise; neither is a medical emergency.
What People Get Wrong
- "My doctor said stop two days before." Two days is not enough for weekly drugs — half-life is 5-7 days. Either hold 7 days under the older rule or follow the 24-hour clear liquid path under the new rule.
- Not telling the anesthesia team. Many people consider weight-loss drugs separate from "real medications." They are not. Disclose every time.
- Stopping liraglutide a week early. Daily drugs only need a 24-hour hold; a one-week hold is unnecessary and worsens glycemic control.
- Assuming "weight-loss dose" means lower aspiration risk. Wegovy 2.4 mg and Ozempic 1 mg are both semaglutide. The gastric effect is dose-related but not absent at lower doses.
- Drinking protein shakes during the clear-liquid prep day. Protein shakes are not clear liquids. Stick to water, clear broth, apple juice, plain tea, black coffee, sports drinks, Jell-O without fruit, popsicles without dairy or fruit pieces.
- Restarting at full dose after 4 weeks off. Tolerance fades quickly. Re-titrate from the starting dose if you have been off more than 2-4 weeks.
Frequently Asked Questions
Do I have to stop Ozempic before a colonoscopy? Not necessarily under 2024 guidance. The AGA-endorsed approach is to continue the drug and follow a 24-hour clear liquid diet before the procedure, with holds reserved for patients in dose escalation, on maximum doses, or with active GI symptoms.
How long before surgery should I stop tirzepatide? If your team is following the 2023 ASA rule, 7 days. If they are using the 2024 multisociety approach, you may be able to continue and instead follow a 24-hour clear liquid diet. Confirm with your anesthesiologist.
How long before surgery should I stop liraglutide or oral semaglutide? Daily-dosed GLP-1s need only a 24-hour hold — skip the dose on the day of the procedure.
What if I forgot and took my GLP-1 the day before surgery? Tell the team. If you have no GI symptoms, the procedure often proceeds with standard precautions, sometimes with a gastric ultrasound or a switch to general anesthesia with rapid sequence intubation.
Can I have my colonoscopy if I took Ozempic that morning? Usually yes, but the team needs to know. Expect a longer fasting window, possible ultrasound, and a discussion about airway plan.
What about a 14-day hold for joint replacement? Some 2025 orthopedic data suggested 14 days may give more reliable gastric clearance for total joint surgery. The 2024 multisociety guidance does not endorse 14 days as standard, but some surgeons request it.
When can I restart after surgery? Once you are eating normally without nausea — typically a few days for minor procedures, 1-2 weeks for major abdominal surgery. Resume your previous dose if off less than 2 weeks; re-titrate from the starting dose if off longer.
Is there really an aspiration risk or is this overblown? The risk is real but small in absolute terms. Case reports and physiology support concern; large observational studies have not shown a major increase in clinical aspiration rates in elective surgery. The 2024 guidance reflects both facts at once.
Last reviewed: May 13, 2026
Sources
- New Multi-Society GLP-1 Guidance (October 2024) — American Society of Anesthesiologists
- Multi-Society Clinical Practice Guidance for the Safe Use of GLP-1 Receptor Agonists in the Perioperative Period — PMC
- ASA Consensus-Based Guidance on Preoperative Management of Patients on GLP-1 Receptor Agonists (June 2023)
- AGA Does Not Endorse All Patients Stopping GLP-1 Drugs Prior to Endoscopy — American Gastroenterological Association
- Drugs for Diabetes or Weight Loss: What to Know Before Surgery — ASA Patient Resources
- Should GLP-1 Receptor Agonists Be Withheld During the Preoperative Period? — Cleveland Clinic Journal of Medicine
- Holding GLP-1 Prior to Colonoscopy: Current Guidelines and Safety — Fella Health
- Perioperative Management of Long-Acting GLP-1 Receptor Agonists — PubMed
- SPAQI Multidisciplinary Consensus Statement on Perioperative GLP-1 Management — PMC