Women now make up the majority of GLP-1 prescriptions in the United States, and their experience on these drugs is not a smaller version of the male experience. Hormones, reproductive biology, perimenopause, and bone health all reshape how a GLP-1 acts in a female body — sometimes for better, occasionally for worse. The PCOS response is striking. The fertility rebound has earned its own nickname. And a handful of women-specific risks deserve more attention than they typically get from prescribers writing the script in five minutes.
Direct answer: For women, GLP-1 receptor agonists (semaglutide, tirzepatide, liraglutide) produce larger absolute weight loss than in men in pooled data but tend to respond slightly slower per milligram of dose. They normalize menstrual cycles in roughly 80% of obese PCOS responders, restore ovulation in many women previously labeled infertile (the "Ozempic babies" phenomenon), deliver approximately 20% weight loss across all menopause stages, show an early breast cancer risk-reduction signal, and provide cardiometabolic and mood benefits that matter especially in perimenopause. They also raise meaningful concerns: oral contraceptive failure during tirzepatide titration, accelerated bone density loss in postmenopausal women, hair shedding in roughly 2% of women (often more after rapid loss), and the cosmetic phenomenon called Ozempic face.
Do Women Lose Weight Differently Than Men?
Yes — in two directions that initially look contradictory.
Total weight loss is larger on average in women. A 2026 meta-analysis of six trials covering 19,906 patients found women on GLP-1 receptor agonists lost about 10.9% of starting weight versus 6.8% in men. Proposed reasons: synergistic interactions with estrogen, slower drug clearance in women, lower median starting body weight (so the same dose hits a smaller person harder), and slightly different fat distribution.
Per-dose response can be slower at any given titration step. Endocrinologists and weight clinics report women often need an extra month at each dose to reach the same tolerability and weekly loss as men. The net trajectory is similar or better, but the early weeks can feel disappointing if a woman is comparing herself to a male partner on the same protocol — which is common, and a known driver of early dropout.
Practical reading: women should expect the scale to be slower for the first 8 to 12 weeks, then accelerate. Comparing your week-six progress to a 200-pound man's week-six progress is not a fair comparison.
PCOS: The Strongest Women-Specific Benefit
Polycystic ovary syndrome affects roughly 8 to 13% of reproductive-age women and is driven by insulin resistance, hyperandrogenism, and irregular ovulation. GLP-1s hit two of those three mechanisms directly.
A 2023 Journal of Clinical Medicine study (Carmina and Longo) treated 27 obese PCOS patients who had failed lifestyle intervention with semaglutide 0.5 mg weekly for 6 months:
- Mean weight loss: 11.5 kg
- Mean BMI dropped from 34.4 to 29.4
- About 80% of responders normalized menstrual cycles
- 71% of the responder cohort achieved fully normal menses
- Fasting glucose normalized in 80% of impaired-fasting-glucose participants
- Only 33% had mild morning nausea; zero withdrawals
Other studies show similar patterns: improved insulin sensitivity, reduced free testosterone, and resumption of ovulation in women who had been anovulatory for years. No GLP-1 is yet FDA approved specifically for PCOS, but it is a rapidly growing off-label indication, and a Phase 3 PCOS trial is recruiting in 2025–2026.
For women whose PCOS has driven a decade of weight gain, irregular cycles, acne, and infertility, the GLP-1 response can feel like the first treatment that actually addressed the metabolic core of the disease.
Perimenopause and Menopause Weight Gain
Estrogen decline in the menopausal transition slows metabolic rate, shifts fat from gluteofemoral to visceral storage, and disrupts sleep — a triad that typically drives ~1.5 kg per year of perimenopausal weight gain, totaling roughly 10 kg by the time menses stop.
GLP-1s work essentially as well in this population:
- SURMOUNT-1 subgroup analysis (tirzepatide): 26% weight loss premenopausal, 23% perimenopausal, 23% postmenopausal, all versus 2–3% placebo
- STEP UP (high-dose semaglutide 7.2 mg): 22.6% premenopausal, 19.7% perimenopausal, 19.8% postmenopausal
- 41% of premenopausal women on STEP UP reached ≥25% body weight loss
Notably, the visceral fat that drives perimenopausal cardiometabolic risk responds particularly well to GLP-1 therapy. Hot flashes, sleep fragmentation, and mood symptoms also improve in many women — partly from weight loss, partly from the drug's direct effects on inflammation and reward signaling. Wegovy with or without menopausal hormone therapy was associated with lower migraine and depression risk than hormone therapy alone in 2026 data from the European Congress on Obesity.
There is no documented negative interaction between GLP-1s and HRT, but the combination should be coordinated by a clinician who is paying attention to both.
Fertility and the "Ozempic Babies" Phenomenon
Obesity reduces fertility by roughly 5% per BMI point above 29, per Dr. Deidre McIntosh and others. GLP-1s lower that BMI — and the result has been a wave of pregnancies in women who had been trying, sometimes for years, to conceive.
What the evidence shows:
- Even modest weight loss restores ovulation in many women with obesity-related anovulation
- Improved insulin signaling lowers free androgens (especially relevant in PCOS)
- Reduced inflammation and improved endometrial environment may improve implantation
- Some women conceive within months of starting therapy after years of infertility
Important warnings, not optional:
- GLP-1s are not approved in pregnancy and animal studies show fetal harm. Stop the medication at least 2 months before conception — the consensus washout — to clear the drug and stabilize nutrition.
- A "barrier or non-oral contraceptive" strategy is essential during titration if pregnancy is unwanted (see contraception section below).
- Improved fertility from a GLP-1 does not equal lifetime fertility restoration. Conception odds normalize, not maximize.
This phenomenon also has a male component: there is preliminary evidence of improved sperm count, concentration, and motility in obese men on GLP-1s, so partners on therapy can both be moving toward conception simultaneously.
Breast Cancer: An Early Risk-Reduction Signal
Postmenopausal women with BMI over 35 face up to a 60% higher risk of invasive breast cancer. Women who lose ≥10 pounds and keep it off have a 32% reduction in future breast cancer risk. GLP-1s achieve both effects routinely.
Preclinical and early clinical data are encouraging:
- Obese mice on GLP-1s developed tumors more slowly; total cancer risk dropped close to lean-mouse baseline
- Approximately 46,000 GLP-1-treated patients showed no increased breast cancer risk versus controls
- Duke and other research groups are studying whether GLP-1s reactivate exhausted obesity-related immune surveillance against tumor cells
- The 2025 San Antonio Breast Cancer Symposium featured multiple sessions on GLP-1s for breast cancer prevention and survivorship
Important caveat: women with active or recent breast cancer were excluded from the major GLP-1 trials, so safety data in that population is thin. Most oncologists currently advise against starting a GLP-1 during active chemotherapy or in the first year after diagnosis — but prevention in high-risk healthy women is a much more open conversation.
Bone Density: A Postmenopausal Concern
This is the most underrecognized women-specific risk on the GLP-1 conversation.
Rapid weight loss reduces mechanical loading on the skeleton, and in postmenopausal women — already losing about 1% bone mineral density per year from estrogen decline — the effect can be additive. 2024–2026 data show:
- About 4% of GLP-1 users developed osteoporosis versus 3% of non-users — roughly a 30% relative increase
- Hip BMD is the most affected site
- 25–40% of weight lost on GLP-1s can come from lean mass without active countermeasures
Mitigation that actually works:
- Resistance training 2–3 times per week — the single most effective intervention; one trial showed exercise plus liraglutide preserved hip, spine, and forearm BMD despite larger weight loss
- Protein at 1.2–1.6 g/kg/day to support muscle and bone matrix
- Calcium 1,000–1,200 mg/day and vitamin D 800–2,000 IU/day
- Baseline DEXA scan for any woman over 50 starting a GLP-1, repeat at 12–24 months
- Slowing the pace of weight loss if BMD is dropping
A woman starting a GLP-1 at age 55 with a family history of osteoporosis should not be doing this without a DEXA and a strength program.
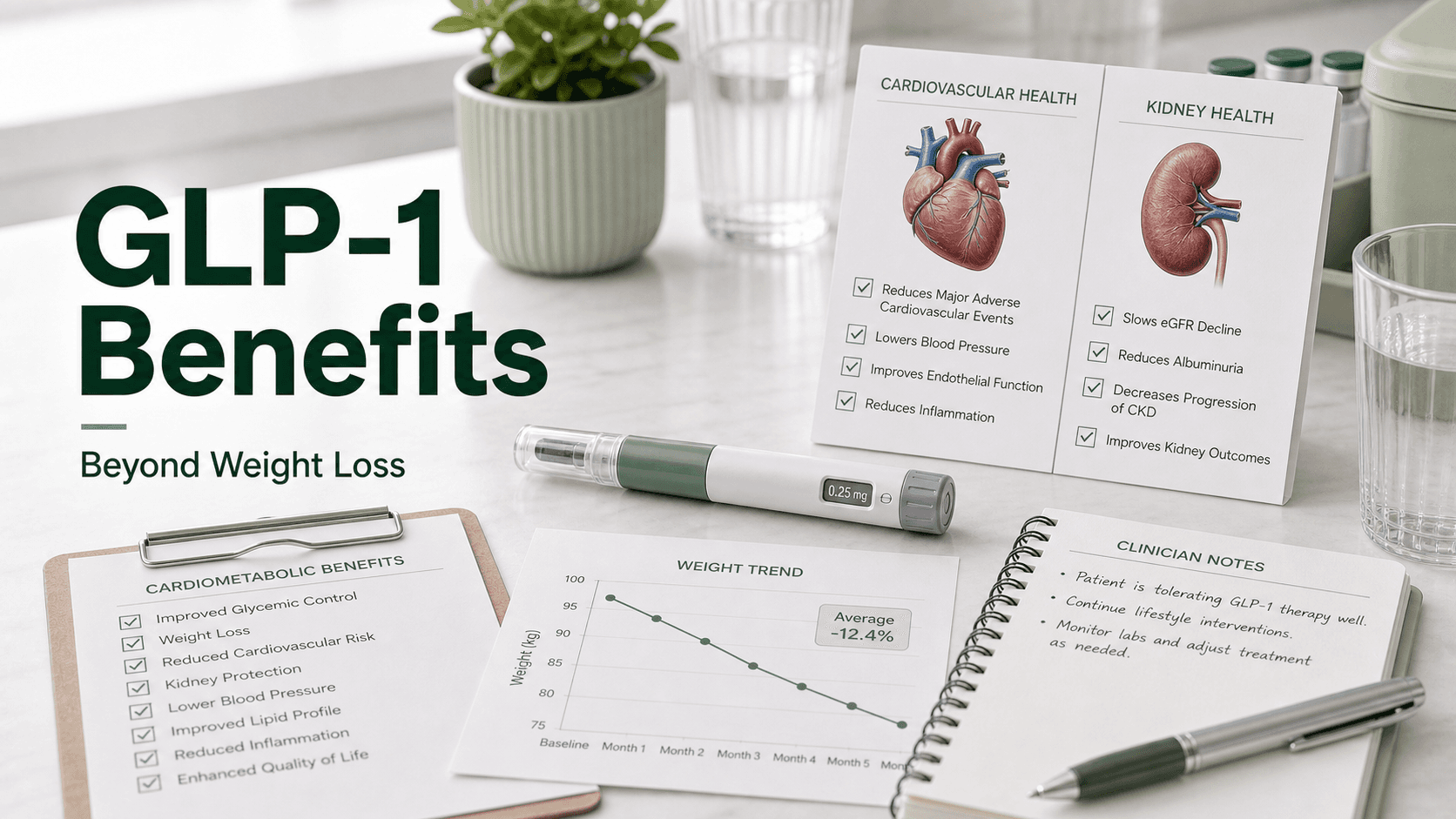
Cardiometabolic Protection
Heart disease is the leading cause of death in women, and women are historically underdiagnosed and undertreated. GLP-1s help close the gap.
- SELECT trial: ~20% reduction in major adverse cardiovascular events in adults with obesity and existing cardiovascular disease (women were 28% of the cohort, with similar effect sizes)
- Blood pressure typically drops 10–15 mmHg systolic
- Triglycerides fall 20–30%; LDL falls 5–10%
- Visceral fat — the perimenopausal driver of cardiometabolic risk — responds preferentially
- A1C improvements of 1–2% for women with type 2 diabetes or prediabetes
Women in perimenopause are exactly the demographic where these effects compound most.
Mental Health and Mood
Depression rates are roughly twice as high in women as men, and both perimenopause and PCOS independently raise risk. GLP-1 effects on mood are mixed but lean positive:
- Multiple 2025–2026 analyses show GLP-1 users have lower or unchanged rates of depression and suicidality compared to matched controls
- Some women report a marked drop in "food noise" that reduces shame, bingeing, and depressive rumination tied to eating
- A subset experiences a flatter affect or anhedonia, possibly from reduced reward signaling — usually mild and reversible
- Anxiety appears to track weight loss progress for most women
The headline FDA warning about suicidality has not been confirmed in large observational data, but a personal history of severe depression warrants closer monitoring during titration.
Hair Loss After Rapid Weight Loss
About 2% of women on GLP-1s experience drug-associated hair loss in clinical reports, with much higher rates in women who lose more than 10% of body weight in 3–6 months — the rapid-loss threshold for telogen effluvium. Some clinic data put the rate at 15–25% among rapid-loss patients, more than double the rate in men.
Key facts:
- Onset is typically 3–6 months after initiating therapy
- It is telogen effluvium (a synchronized shedding phase), not androgenic loss — so it is almost always reversible
- Iron deficiency and low protein worsen it; both are common in women who eat poorly under appetite suppression
- Recovery usually starts within 6 months even on continued GLP-1 therapy
Mitigation: protein at 1.2–1.6 g/kg/day, iron and ferritin checks, biotin if low, slower titration if shedding is severe.
Ozempic Face
Rapid loss of facial fat creates the gauntness, hollowing, and skin laxity now called Ozempic face. The drug itself does not cause skin changes; the rate of loss does. Women report it more often than men, both because they lose more total weight on average and because facial cosmetic outcomes are scrutinized more.
Prevention is mostly about pace: aim for slow, steady loss over 12–18 months rather than racing to 20% in 6 months. Strength training, adequate protein, and dermatologic interventions (fillers, biostimulators, retinoids, sunscreen) can manage the cosmetic side without stopping therapy.
Contraception: The Underdiscussed Interaction
This one is medically important and routinely missed in primary care.
Tirzepatide reduces the peak plasma concentration of ethinyl estradiol by 59% and norgestimate by 66% when an oral contraceptive is co-administered. The interaction is mechanical (delayed gastric emptying altering absorption), not metabolic. Semaglutide has a milder but still real effect.
Eli Lilly's prescribing recommendation for Zepbound and Mounjaro:
Switch to a non-oral contraceptive method, or add a barrier method, for 4 weeks after starting tirzepatide and for 4 weeks after each dose escalation.
Unaffected methods: IUDs (hormonal or copper), implants, injections, patches, vaginal rings. Affected method: oral pills (combination or progestin-only).
If pregnancy is unwanted, this is not optional. A meaningful share of Ozempic babies are women who did not know about this interaction.
What People Get Wrong About GLP-1s in Women
- "Women just lose less weight on these drugs." False. Women lose more on average; they sometimes progress slower per dose.
- "GLP-1s cause infertility." The opposite, in most cases — they restore fertility in obesity and PCOS. They must be stopped before pregnancy, but they are not anti-fertility drugs.
- "Menopause makes GLP-1s ineffective." Untrue. Postmenopausal weight loss is within a couple of points of premenopausal results.
- "Bone loss is just from the drug." It is mostly from the rate of weight loss and undertrained skeleton — both fixable.
- "Hair loss is permanent." It is almost always telogen effluvium and reverses within 6–12 months.
- "Ozempic doesn't interact with the pill." Tirzepatide absolutely does. Use a non-oral or backup method during titration.
- "Breast cancer survivors should never take a GLP-1." Not the consensus — but it requires an oncology conversation.
Frequently Asked Questions
Do women lose less weight on GLP-1s than men? On average women lose more total weight than men on the same drug (about 10.9% vs 6.8% in pooled meta-analysis), but per-dose response can be slower in the first 8–12 weeks of titration.
Can GLP-1s treat PCOS? Yes, off-label. A 2023 study showed about 80% of obese PCOS responders normalized menstrual cycles on low-dose semaglutide, with significant weight loss and improvements in insulin resistance and androgens.
What is an Ozempic baby? An unexpected pregnancy in a woman taking a GLP-1, often after years of infertility tied to obesity or PCOS. Mechanism is restored ovulation plus possible birth control absorption issues.
Should I stop my GLP-1 before trying to conceive? Yes. Stop at least 2 months before trying to get pregnant. The drugs are not approved in pregnancy and animal data show potential fetal risk.
Does tirzepatide affect birth control pills? Yes. Use a non-oral contraceptive method or add a barrier method for 4 weeks after starting and 4 weeks after each dose escalation. IUDs, implants, injections, patches, and rings are unaffected.
Do GLP-1s cause bone loss in postmenopausal women? Some — observational data show roughly 30% higher osteoporosis incidence in users, driven mostly by rapid weight loss and lean mass loss. Resistance training, protein, calcium, vitamin D, and a baseline DEXA are the standard mitigation.
Will a GLP-1 work during menopause? Yes. Weight loss is approximately 20% across premenopausal, perimenopausal, and postmenopausal women in SURMOUNT-1 and STEP UP subgroups.
Why am I losing hair on a GLP-1? Telogen effluvium triggered by rapid weight loss (over 10% in 3–6 months) and frequently worsened by low protein or low iron. It almost always reverses within 6–12 months. Maintain protein, check iron and ferritin, and slow the pace if needed.
Are GLP-1s safe with HRT? There is no documented negative interaction between semaglutide or tirzepatide and standard menopausal hormone therapy. Coordinate with a prescriber familiar with both.
Do GLP-1s reduce breast cancer risk? Early observational and preclinical data are encouraging, with no increased risk in ~46,000 GLP-1-treated patients and meaningful reductions in tumor development in animal models. Definitive prevention trials are pending.
Last reviewed: May 13, 2026
Sources
- 'Ozempic Babies': How GLP-1 Agonists Affect Fertility — Cleveland Clinic
- Women in Menopause Benefit From GLP-1 Weight-Loss Medications as Much as Younger Women — NewYork-Presbyterian
- Semaglutide Treatment of Excessive Body Weight in Obese PCOS Patients Unresponsive to Lifestyle Programs — Carmina & Longo, J. Clin. Med. 2023
- GLP-1 Weight Loss Higher Among Women — Medscape
- The Impact of Tirzepatide and Glucagon-Like Peptide 1 Receptor Agonists on Oral Hormonal Contraception — JAPhA
- What You Need to Know About GLP-1s and Breast Cancer Care — Breast Cancer Research Foundation
- GLP-1s May Increase Risk of Osteoporosis and Gout, New Research Finds — NBC News
- Hair Loss Associated With Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists — PMC
- 'Ozempic Face': What It Is and How to Avoid It — Cleveland Clinic
- Wegovy Delivered Substantial Weight Loss in Women Across All Menopause Stages — Novo Nordisk / BioSpace