


GLP-1 Qualifications: Who Actually Qualifies in 2026
GLP-1 qualification is two separate questions. The first is whether the FDA-approved label fits you. The second — usually harder — is whether your insurance company will pay for it. The label criteria are written by the agency that approved the drug. The insurance criteria are written by people whose job is to limit spend. Mixing them up is the most common reason people think they "don't qualify" when they actually do, and vice versa.
Eligibility can differ if you have had weight-loss surgery; see using a GLP-1 after gastric bypass.
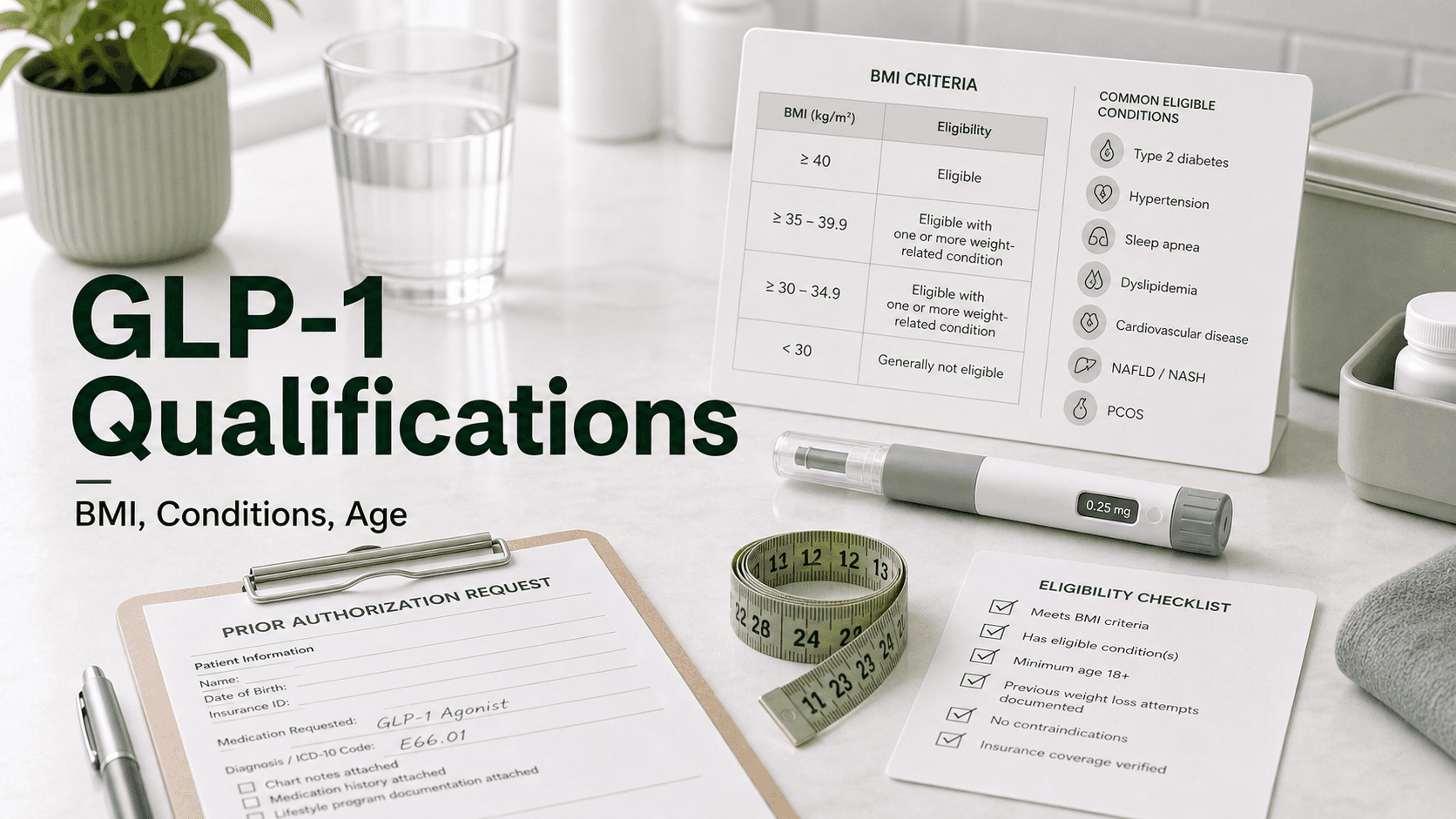
Direct answer: Under FDA labeling for chronic weight management, adults qualify for a GLP-1 with a BMI of 30 kg/m² or higher, OR a BMI of 27 kg/m² or higher with at least one weight-related condition (hypertension, type 2 diabetes, dyslipidemia, obstructive sleep apnea, established cardiovascular disease, or MASH). Wegovy and Saxenda are also approved from age 12; Zepbound, oral Wegovy, and Foundayo are adults only (18+). Insurance plans typically apply the same BMI rule but add: documented BMI history, a 3–6 month supervised lifestyle attempt, and in many cases a prior failed trial of metformin (for Ozempic/Mounjaro under a diabetes indication).
FDA-Approved Qualification Criteria
These are the rules written on the prescribing label. A licensed prescriber can write the prescription if you meet them — independent of whether insurance will cover it.
Adult BMI Criteria (all weight-management GLP-1s)
| BMI | Additional requirement | Qualifies? |
|---|---|---|
| ≥30 kg/m² (obesity) | None — BMI alone is enough | Yes |
| 27–29.9 kg/m² (overweight) | At least one weight-related condition | Yes |
| 25–26.9 kg/m² | Not in label for weight management | Generally no |
| <25 kg/m² | Healthy weight range | No |
Two label updates are worth knowing. In March 2024 (semaglutide) and October 2024 (tirzepatide), the FDA refined the indication language to "adults with obesity, or adults with overweight in the presence of at least one weight-related comorbid condition." The 30/27 BMI thresholds are still how clinicians and insurers operationalize this in practice.
Drug-Specific FDA Indications
| Drug | Primary indication | Minimum age |
|---|---|---|
| Wegovy (semaglutide injection) | Chronic weight management; CV risk reduction in established CVD | 12 |
| Wegovy (oral semaglutide) | Chronic weight management in adults | 18 |
| Zepbound (tirzepatide) | Chronic weight management; moderate-to-severe OSA with obesity | 18 |
| Saxenda (liraglutide) | Chronic weight management | 12 |
| Ozempic (semaglutide) | Type 2 diabetes; CV risk reduction; CKD progression in T2D | 18 |
| Mounjaro (tirzepatide) | Type 2 diabetes | 18 |
| Rybelsus (oral semaglutide) | Type 2 diabetes | 18 |
| Foundayo (oral semaglutide low-dose) | Chronic weight management | 18 |
What Counts as a "Weight-Related Condition"
For the BMI 27 pathway, the FDA recognizes a defined set of weight-related comorbidities. Insurance prior authorization forms ask for documentation — an ICD-10 code, a recent lab, or a sleep study, not a self-report.
- Type 2 diabetes — A1C ≥6.5%, fasting glucose ≥126 mg/dL on two occasions, OGTT 2-hour ≥200 mg/dL, or random glucose ≥200 mg/dL with symptoms.
- Prediabetes — A1C 5.7–6.4% or fasting glucose 100–125 mg/dL. Accepted under Medicare's Bridge program and many commercial plans.
- Hypertension — Diagnosed and either treated or with documented BP ≥130/80 mmHg.
- Dyslipidemia — LDL elevated, low HDL, or elevated triglycerides; can be treated or untreated.
- Obstructive sleep apnea — Confirmed by polysomnography or home sleep study with AHI ≥15 events per hour (Zepbound's standalone OSA indication uses this threshold).
- Established cardiovascular disease — Prior MI, prior stroke, symptomatic peripheral artery disease, or angiographic CAD.
- MASH (metabolic dysfunction–associated steatohepatitis) — Biopsy-confirmed or imaging-supported in many newer payer policies.
- Heart failure with preserved ejection fraction (HFpEF) in patients with obesity — Increasingly accepted following the STEP-HFpEF trials.
- Osteoarthritis with weight-bearing impact — Less universally accepted, but qualifies under some plans.
- PCOS with metabolic features — Often accepted as a documented comorbidity, though not on every plan's list.
A "weight-related condition" you saw on a list ten years ago — like gallbladder disease, GERD, or stress incontinence — is generally not enough on its own for current insurance criteria. The big six (T2D, HTN, dyslipidemia, OSA, CVD, MASH) cover almost every approved case.
Insurance Prior Authorization Criteria
This is where most qualified-on-paper patients hit a wall. Insurance criteria layer additional requirements on top of FDA labeling. The most common stack:
- Documented BMI history, often two readings over 6 months, in the chart.
- 3–6 months of supervised lifestyle intervention — diet program, behavioral counseling, or medically supervised weight management, with documentation from a dietitian, weight-loss clinic, or primary care.
- For diabetes indications: a prior trial of metformin, typically 3 months at a tolerated dose, before semaglutide or tirzepatide for T2D.
- For weight indications: a prior trial of phentermine, orlistat, or another covered weight medication on some restrictive formularies.
- Comorbidity documentation: a recent lab, sleep study, or ICD-10 code for the qualifying condition.
- Ongoing program participation during therapy and ≥5% weight loss at reauthorization (usually 6–12 months in).
A few realities of 2026 PA:
- Many large insurers tightened — not loosened — criteria for the 2026 plan year. Several stopped grandfathering existing approvals at group anniversaries.
- Decisions usually come within 3–7 business days. Standard appeal windows are 30–60 days; over 65% of commercial appeals for GLP-1s succeed when properly documented.
- Medicare Part D historically did not cover weight-loss GLP-1s. CMS's GLP-1 Bridge demonstration runs July 1, 2026 to December 31, 2027 and offers access to Medicare Part D beneficiaries who are 18+ with BMI ≥27 and at least one of: prediabetes, prior MI, prior stroke, or symptomatic PAD.
- Ozempic and Mounjaro for off-label weight loss without a T2D diagnosis are almost universally denied by commercial insurers.
Age Eligibility, Including Pediatric
Age cutoffs depend on the drug and the indication, not the class.
- Wegovy (subcutaneous semaglutide) — approved from age 12 for adolescents with a BMI at or above the 95th percentile on age- and sex-specific growth charts (the clinical definition of pediatric obesity).
- Saxenda (liraglutide) — approved from age 12 with body weight >60 kg (132 lb) and a BMI corresponding to adult BMI ≥30.
- Zepbound (tirzepatide) — adults 18+ only; pediatric safety and efficacy not yet established.
- Oral Wegovy — adults 18+ only.
- Ozempic, Mounjaro, Rybelsus, Foundayo — adults 18+ only.
For adolescents, providers also weigh psychosocial readiness, family support, and growth trajectory. Adolescent prescribing typically happens inside a pediatric obesity program, not as a one-visit refill from urgent care.
Contraindications That Override Qualification
Meeting BMI and comorbidity criteria does not override absolute contraindications. The class-wide list includes personal or family history of medullary thyroid carcinoma (MTC), multiple endocrine neoplasia type 2 (MEN2), prior anaphylaxis or angioedema to a GLP-1, pregnancy, and active breastfeeding. Relative contraindications — pancreatitis history, severe gastroparesis, active proliferative retinopathy — usually trigger a discussion rather than an automatic no.
See the full breakdown: GLP-1 contraindications: the complete absolute and relative list.
BMI Quick Reference
BMI is weight in kilograms divided by height in meters squared, or — in US units — weight in pounds × 703, divided by height in inches squared.
| Height | BMI 27 starts at | BMI 30 starts at |
|---|---|---|
| 5'0" (60 in) | 138 lb | 153 lb |
| 5'2" (62 in) | 148 lb | 164 lb |
| 5'4" (64 in) | 157 lb | 175 lb |
| 5'6" (66 in) | 167 lb | 186 lb |
| 5'8" (68 in) | 177 lb | 197 lb |
| 5'10" (70 in) | 188 lb | 209 lb |
| 6'0" (72 in) | 199 lb | 221 lb |
| 6'2" (74 in) | 210 lb | 233 lb |
If you are within 5 lb of the threshold, ask for two BMI measurements in your chart over 4–6 months — many PA forms accept the higher reading or the average.
If You Don't Qualify
Not qualifying today is not necessarily a permanent answer. Options grouped by likely usefulness:
- Document your BMI trend. If you are at BMI 26 and gaining, two consecutive readings at 27+ over a few months will move you onto the BMI 27 pathway if a comorbidity is also present.
- Get the comorbidity worked up. Many patients who think they have only weight as a problem have undiagnosed prediabetes, dyslipidemia, hypertension, or OSA. A standard panel plus a screening sleep study identifies a qualifying comorbidity in a large share of cases.
- Use a covered alternative. Bupropion-naltrexone (Contrave), phentermine-topiramate (Qsymia), and orlistat are FDA-approved for the same BMI thresholds and are sometimes covered when GLP-1s are not. Metformin, while not a weight-loss drug, has modest weight effects and is widely covered.
- Bariatric surgery referral. BMI ≥40 alone, or BMI ≥35 with comorbidity, qualifies for bariatric surgery under most commercial plans and Medicare. Some payers cover surgery before GLP-1.
- Cash-pay branded. Both Lilly (Zepbound vials) and Novo Nordisk (Wegovy direct) offer cash-pay channels at ~$349–$499/month as of 2026. No insurance criteria apply.
- Lifestyle program with a downstream PA path. Enrolling in a supervised program now creates the 3–6 month lifestyle documentation many plans require — useful even if you intend to push for a GLP-1 later.
What People Get Wrong About Qualifying
- "My BMI is 26 so I cannot qualify." Correct under current FDA labeling, but only just. Many patients qualify within months of intentional weight gain, growth, or a re-check with calibrated equipment. More importantly, a documented comorbidity is the bigger lever.
- "My doctor said I'm healthy so I do not qualify." Healthy on a snapshot may still mean prediabetic, dyslipidemic, or apneic on workup. Ask for a full lipid panel, A1C, and OSA screening if BMI is in the 27–29 range.
- "Ozempic is denied so all GLP-1s are denied." Ozempic for off-label weight loss is denied; Wegovy or Zepbound for chronic weight management is a separate PA pathway.
- "My adolescent cannot take a GLP-1." Wegovy and Saxenda are approved from age 12 with adolescent obesity criteria.
- "I failed metformin so I don't qualify." The opposite — failing metformin is usually the step therapy gate that lets you onto a GLP-1 for T2D.
- "Medicare doesn't cover GLP-1s." True historically. The GLP-1 Bridge demonstration opens July 1, 2026 for eligible Part D beneficiaries with prediabetes or cardiovascular disease.
Frequently Asked Questions
What is the minimum BMI for a GLP-1? 27 kg/m² with at least one weight-related condition, or 30 kg/m² with no other requirement.
Does prediabetes count as a comorbidity? Under the FDA's weight-management label, the recognized conditions are obesity-related (HTN, T2D, dyslipidemia, OSA, CVD, MASH). Prediabetes alone is not in the original FDA label, but is accepted by many commercial plans and by Medicare's Bridge demonstration.
Do I need to fail metformin first? For Ozempic or Mounjaro under a T2D indication, most insurers require a 3-month metformin trial. For Wegovy or Zepbound under a weight-management indication, metformin failure is not standard.
Does insurance require a lifestyle program? Most plans require 3–6 months of documented supervised lifestyle intervention. This can be a dietitian, behavioral counseling, or a medically supervised weight management program.
Can teenagers qualify? Yes for Wegovy and Saxenda from age 12, with a BMI at or above the 95th percentile. Zepbound is adults only.
What if my BMI is 26? You generally do not qualify under FDA labeling. Consider documenting BMI over time, getting a full metabolic and OSA workup, and discussing alternatives like Contrave or Qsymia.
Does Medicare cover GLP-1s for weight loss in 2026? Standard Part D does not. The CMS GLP-1 Bridge demonstration provides time-limited access from July 1, 2026 through December 31, 2027 to eligible beneficiaries 18+ with BMI ≥27 and prediabetes, prior MI, prior stroke, or symptomatic PAD.
How long does prior authorization take? Typically 3–7 business days for an initial decision. Appeals are decided within 30–60 days and succeed about 65% of the time when properly documented.
Can I qualify on cash-pay if insurance denies me? Yes. Lilly Direct (Zepbound vials) and NovoCare (Wegovy direct) bypass insurance criteria entirely. The qualification floor is still the FDA-approved indication.
Last reviewed: May 13, 2026
Sources
- Wegovy Prescribing Information — FDA accessdata
- Zepbound Prescribing Information — FDA accessdata
- Medicare GLP-1 Bridge — CMS
- FDA Approves Zepbound for Moderate-to-Severe OSA — FDA
- Wegovy for Adolescents — Novo Nordisk
- GLP-1 Medications for Weight Loss: How to Get Started — Yale Medicine
- Qualifying for GLP-1 Weight Loss — Hopkins MD
- Zepbound Prior Authorization Criteria 2026 — Honest Care
- Ozempic Prior Authorization Criteria — Klarity
- GLP-1 Receptor Agonists for Obesity: Eligibility Across 99 Countries — Lancet Diabetes & Endocrinology
- Changes Are Coming: Medicare Access to GLP-1 Medications — Obesity Action Coalition




