Bariatric surgery is the most effective obesity treatment ever invented, and it still isn't a cure. Roughly one in five sleeve and bypass patients never reaches expected weight loss, and a larger group regains a meaningful share of what they lost within five to ten years. GLP-1 medications are now the most studied tool for that second chapter — not as a replacement for surgery, but as a layer on top of it.
Direct answer: Most bariatric programs in 2026 add a GLP-1 (semaglutide, Wegovy, or tirzepatide) at least 12 months after surgery, once weight loss has plateaued or regain has started. In published cohorts, post-bariatric patients lose an additional 5–15% of total body weight on a GLP-1, with semaglutide and tirzepatide outperforming liraglutide. The randomized BARI-OPTIMISE trial showed 8.8% loss on liraglutide vs 0.5% on placebo in patients with poor surgical response. Injectable semaglutide and tirzepatide are strongly preferred over oral semaglutide after gastric bypass because oral absorption depends on intact stomach anatomy.
Why Patients Pursue GLP-1 After Bariatric Surgery
The early years after bariatric surgery look spectacular for most patients. Then biology pushes back.
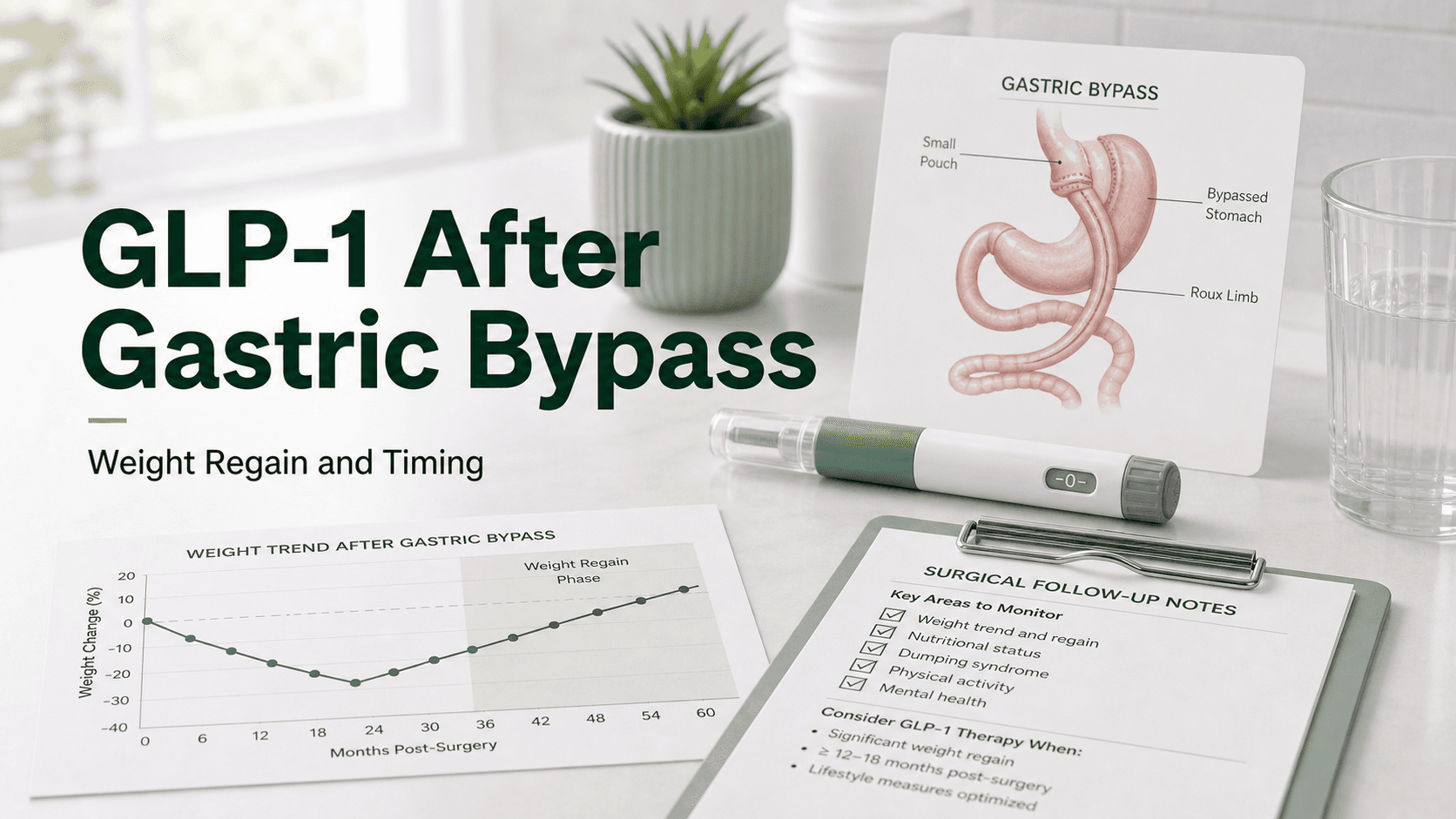
- Weight regain after sleeve gastrectomy: typically 15–25% of nadir weight by year 5, with continued slow drift after that.
- Weight regain after Roux-en-Y gastric bypass: typically 10–20% of nadir weight by year 5.
- Insufficient initial weight loss: roughly 20% of patients never hit the expected 20%+ TBWL benchmark, often called "low responders."
- One in seven bariatric patients eventually seeks pharmacotherapy years after their original procedure.
Three patterns drive most referrals for a GLP-1 after surgery:
- Weight regain. The pouch dilates, hunger hormones renormalize, and a few hundred extra daily calories accumulate quietly.
- A plateau short of goal. A bypass patient who lost 25% but needs to lose 35% for joint, sleep apnea, or fertility reasons.
- Recurrence of metabolic disease. Diabetes, hypertension, or fatty liver return even when weight has only mildly regained.
Post-bariatric biology also has a specific deficit that makes a GLP-1 mechanistically appealing. Patients who regain weight after gastric bypass show lower postprandial GLP-1 levels than peers who maintained loss. Adding an exogenous GLP-1 receptor agonist directly restores the missing signal.
The BARI-OPTIMISE Trial
BARI-OPTIMISE is the first randomized controlled trial of a GLP-1 specifically in post-bariatric patients with poor surgical response.
- Population: 70 adults with less than 20% weight loss at least one year after gastric bypass or sleeve gastrectomy.
- Intervention: Liraglutide 3.0 mg daily plus a calorie-reduced diet and exercise, vs placebo, for 24 weeks.
- Result: Mean weight loss of 8.8% on liraglutide vs 0.5% on placebo.
That is roughly eight extra percentage points of total body weight in patients who had previously stalled on surgery alone. The follow-up BARI-STEP trial is testing weekly semaglutide 2.4 mg in the same population and is expected to produce larger numbers, given semaglutide's general superiority to liraglutide in primary obesity trials.
A retrospective European cohort published in 2023 helps calibrate expectations for the modern drugs:
- Liraglutide 3.0 mg: 7.3% total body weight loss, 31% of patients reached 10%+ loss.
- Semaglutide 1.0 mg weekly: 9.8% total body weight loss, 48% of patients reached 10%+ loss.
- Semaglutide 2.4 mg weekly (Wegovy): observational reports of 10–15% additional loss at one year.
- Tirzepatide 10–15 mg weekly: observational reports of 12–18% additional loss at one year, the highest of any post-bariatric GLP-1 series so far.
The honest summary: GLP-1s reliably restart weight loss after surgery, with semaglutide and tirzepatide pulling clearly ahead of older agents.
Efficacy by Procedure Type
Most early data pooled all bariatric procedures together. Newer cohorts break it apart.
Sleeve gastrectomy. Sleeve patients tend to regain more weight, more quickly, than bypass patients. They also tend to respond very well to a GLP-1, partly because the sleeve mostly affects volume and ghrelin, leaving GLP-1 receptor biology largely untouched. Typical additional loss on semaglutide or tirzepatide: 8–15% of total body weight.
Roux-en-Y gastric bypass. Bypass patients already have surgically amplified GLP-1 release. Adding a GLP-1 RA still helps, especially in low responders and patients with regain. Typical additional loss: 6–13% of total body weight. Bypass patients are also more likely to experience dumping-like symptoms with a GLP-1 because of the combined effect on gastric emptying and rapid small-bowel delivery.
Duodenal switch and SADI. Fewer data exist because these patients regain less often. When they do, a GLP-1 is generally well-tolerated, but malabsorption already increases nutritional risk and protein and micronutrient monitoring becomes essential.
Adjustable gastric band. A band that has been removed or no longer functions effectively leaves the patient with native anatomy, so the GLP-1 response resembles a non-surgical patient: roughly 12–20% TBWL depending on the drug.
A retrospective study comparing sleeve-to-bypass conversion against sleeve-plus-GLP-1 in regainers found the medication arm produced comparable weight loss to a revisional operation, without the operative risk. For many patients, a GLP-1 is now the preferred next step before a revisional surgery is considered.
When To Start After Surgery
Almost every bariatric program in 2026 waits a minimum window before starting a GLP-1.
- Earliest reasonable start: 6 months post-op, only in very specific cases (e.g., diabetes that did not remit, severe sleep apnea, insufficient early response).
- Typical start: 12 months post-op, after the natural weight-loss curve has flattened.
- Most common start: 2–6 years post-op, with the fourth year showing the highest initiation rate in registry data.
Why the wait?
- Surgery does most of the work in year one. Adding a GLP-1 during the steep loss phase obscures who is responding to what and risks excessive nutritional compromise.
- Nausea, vomiting, and dehydration are already common after bariatric surgery. A GLP-1 amplifies all three.
- Protein intake is fragile in the first 6–12 months. Anything that suppresses appetite further can push patients below the 60–90 g/day protein floor they need to preserve lean mass.
- The plateau itself is diagnostic. Surgeons want to see where you naturally stabilize before adding a second tool.
Most programs require a formal evaluation before starting: an upper GI series or endoscopy to confirm anatomy, nutrition labs (iron, B12, folate, vitamin D, protein), and a dietitian-led review of eating patterns. If pouch dilation or a fistula is found, surgical revision may come first.
Oral Semaglutide Considerations After Bypass
Oral semaglutide (Rybelsus) is the only oral GLP-1 on the U.S. market, and it does not belong on most post-bypass medication lists.
The tablet relies on a co-formulant called SNAC (sodium N-(8-[2-hydroxybenzoyl] amino) caprylate) that temporarily lowers gastric pH and increases stomach lining permeability to allow the peptide into the bloodstream. Absorption is heavily concentrated in the stomach itself, not the small intestine.
After gastric bypass:
- The functional stomach pouch is roughly 30 mL instead of 1,000–1,500 mL.
- Food and any tablet leave the pouch in minutes and bypass the duodenum entirely.
- Gastric acid is lower because most of the acid-producing cells have been bypassed.
That combination removes nearly every condition oral semaglutide was designed for. No published pharmacokinetic study has confirmed adequate bioavailability after bypass, and most obesity specialists treat oral semaglutide as unreliable in this population.
After sleeve gastrectomy, the stomach is smaller but still acidic and intact. Oral semaglutide may absorb, but data are limited and timing/empty-stomach rules become harder to follow when meal volumes are tiny. Injectable formulations remain the default.
Practical guidance: if you are post-bypass and a clinician prescribes oral semaglutide, ask why injectable wasn't chosen first. After sleeve, oral semaglutide is reasonable to try but expect inconsistent results.
Dose Modifications
Post-bariatric patients tolerate GLP-1s differently than non-surgical patients. Almost every published protocol uses slower titration than the standard label.
Semaglutide (Wegovy):
- Start at 0.25 mg weekly as labeled.
- Extend each step to 6–8 weeks instead of 4 if nausea, vomiting, or volume intolerance occurs.
- Many patients respond well at 1.0–1.7 mg and never need the full 2.4 mg dose.
Tirzepatide (Zepbound):
- Start at 2.5 mg weekly.
- Slow titration to 5 mg and 7.5 mg with at least 6 weeks per step.
- Final dose typically 7.5–12.5 mg; the 15 mg dose is reached less often than in non-surgical patients.
Liraglutide (Saxenda):
- Daily injection; less popular now because of dosing burden and inferior efficacy.
- Useful when weekly drugs are unavailable or unaffordable.
The principle is the same across drugs: titrate by tolerability, not by the calendar. Hitting the highest dose is not the goal — sustainable food intake and adequate protein are.
Side Effect Considerations
Most post-bariatric side effects overlap with non-surgical patients, but a few deserve extra weight.
- Nausea and vomiting are more common and longer-lasting because gastric emptying is already altered.
- Dehydration risk is amplified by smaller fluid capacity per sip. Aim for 64+ oz daily and use electrolyte mixes during titration.
- Protein intake can collapse below the 60–90 g/day floor. Pre-plan three to four protein-anchored meals or shakes.
- Hypoglycemia is uncommon but real, especially in bypass patients who already have post-prandial hypoglycemia.
- Gallstones are elevated after both rapid bariatric loss and GLP-1 therapy; combining the two increases risk further.
- Sarcopenia. Resistance training and protein targets matter even more than usual.
- Reflux can worsen, particularly after sleeve gastrectomy.
Stop the medication and contact your team for: persistent vomiting beyond 48 hours, severe upper abdominal pain (consider pancreatitis or gallstones), inability to maintain hydration, or signs of bowel obstruction.
Insurance and Coverage Challenges
Post-bariatric GLP-1 coverage is the single biggest practical barrier most patients hit.
- Commercial insurance: many plans exclude weight-loss medications entirely, even when bariatric surgery was covered.
- Indication mismatch: Wegovy and Zepbound are labeled for obesity (BMI ≥30, or ≥27 with comorbidity). After successful surgery, BMI may be below 30 and below 27, disqualifying the patient from on-label coverage.
- Type 2 diabetes pathway: if diabetes returns or persists, Ozempic or Mounjaro can be approved through the diabetes benefit, which is more commonly covered.
- Cash-pay options: Lilly Direct (Zepbound vials), Novo Care (Wegovy), and 503A compounded options have made coverage less binary in 2026.
A common workflow: use the diabetes-coded prescription if diabetes is present, document weight regain to justify a higher-BMI threshold when applicable, and use cash-pay or compounded options as a bridge if denied. Bariatric centers typically have prior-authorization teams that handle this well — ask before you pay out of pocket.
What People Get Wrong
- "GLP-1s mean my surgery failed." They don't. Bariatric surgery is a one-time intervention on a chronic disease. Adding pharmacotherapy is treating the disease, not relitigating the operation.
- "I have to wait two years." Most programs allow GLP-1 use after 12 months, and some allow it at 6 months in specific cases.
- "Oral semaglutide is easier than an injection." After bypass, it is also unreliable. Most specialists default to injectable.
- "The highest dose is the goal." Half of post-bariatric patients respond well below the top dose.
- "GLP-1s ruin bariatric surgery results." Combined data show no harm to surgical outcomes and meaningful additional loss in regainers.
- "If a GLP-1 works, I can stop after I hit goal." Like primary obesity treatment, regain is the default after stopping. Long-term, often lifelong, use is the most likely path.
- "Compounded semaglutide is fine after bypass." Possibly — but quality varies. Use a 503A or 503B pharmacy with documented sterility, and inform your bariatric team.
Frequently Asked Questions
How long after gastric bypass can I start a GLP-1? Most surgeons recommend at least 12 months post-op. A minority allow 6 months for diabetes that didn't remit or severe early plateau.
Will a GLP-1 work after gastric sleeve? Yes — sleeve patients generally respond very well, with 8–15% additional total body weight loss on semaglutide or tirzepatide.
How much weight can I lose with a GLP-1 after bariatric surgery? Typical reported ranges are 5–15% additional total body weight, depending on drug and dose. Tirzepatide tends to lead, semaglutide is close behind, liraglutide trails.
Can I take Rybelsus (oral semaglutide) after gastric bypass? Most specialists advise against it because absorption depends on intact stomach anatomy. Injectable semaglutide or tirzepatide is preferred.
Do I need a lower GLP-1 dose after bariatric surgery? Often yes — many post-bariatric patients respond at sub-maximal doses (semaglutide 1.0–1.7 mg or tirzepatide 7.5–12.5 mg). Slower titration is also common.
Is it safe to take Ozempic after gastric bypass? Yes, when prescribed and monitored by an experienced clinician. Side effects can be amplified, so titrate slowly and monitor protein, hydration, and vitamin labs.
Does insurance cover GLP-1s after weight loss surgery? It varies. Diabetes-coded prescriptions (Ozempic, Mounjaro) are more commonly covered than weight-loss-coded ones (Wegovy, Zepbound). Many post-bariatric patients use cash-pay or compounded options.
Will I regain weight if I stop the GLP-1? Most likely yes. Trial data in non-surgical patients show roughly two-thirds of lost weight returns within a year of stopping, and there is no evidence post-bariatric patients are exempt.
Should I get a revisional surgery or a GLP-1 first? Most programs now try a GLP-1 first because it is less invasive and often produces equivalent additional loss. Revision is reserved for anatomic problems (fistula, dilated pouch, severe reflux) or non-responders.
Last reviewed: May 13, 2026
Sources
- Liraglutide for weight regain after metabolic surgery (BARI-OPTIMISE) — Nature Medicine summary
- Post metabolic bariatric surgery weight regain: the importance of GLP-1 levels — International Journal of Obesity
- Glucagon-like peptide-1 receptor agonists for post-bariatric surgery weight regain and insufficient weight loss: a systematic review — Surgery for Obesity and Related Diseases
- Efficacy of liraglutide and semaglutide for weight regain after bariatric surgery: a retrospective observational study — Obesity Surgery (PMC)
- The GLP-1 Era: What Comes After Bariatric Surgery? — PMC review
- GLP-1s for Weight Loss and Maintenance Post-Bariatric Surgery — MedCentral
- Navigating weight loss: When to consider bariatric surgery after GLP-1 therapy — UChicago Medicine
- Sleeve-to-bypass conversion vs. sleeve-with-adjuvant GLP-1 receptor agonists — Surgery for Obesity and Related Diseases
- Why More Bariatric Patients Are Starting GLP-1 Therapy Years After Surgery — Thomas Bariatrics
- Ozempic After Gastric Bypass: Safety, Effectiveness and NHS Guidance — Bolt Pharmacy
- Wegovy After Roux-en-Y Gastric Bypass: absorption, efficacy, and clinical considerations — Pharmacy UK
- Can you take Wegovy (semaglutide) after gastric bypass surgery? — Form Health
- Semaglutide 2.4mg for Low Responders After Bariatric Surgery (BARI-STEP) — ClinicalTrials.gov
- Pharmacotherapy and metabolic/bariatric surgery: either or both? — International Journal of Obesity