


Bariatric surgery has been the most effective obesity treatment for two decades. Then GLP-1s arrived, and the conversation changed. By 2026, GLP-1 prescriptions outnumber bariatric procedures roughly 35 to 1 in the United States. Yet head-to-head data still favors surgery on the two outcomes that matter most: absolute weight loss and durability.
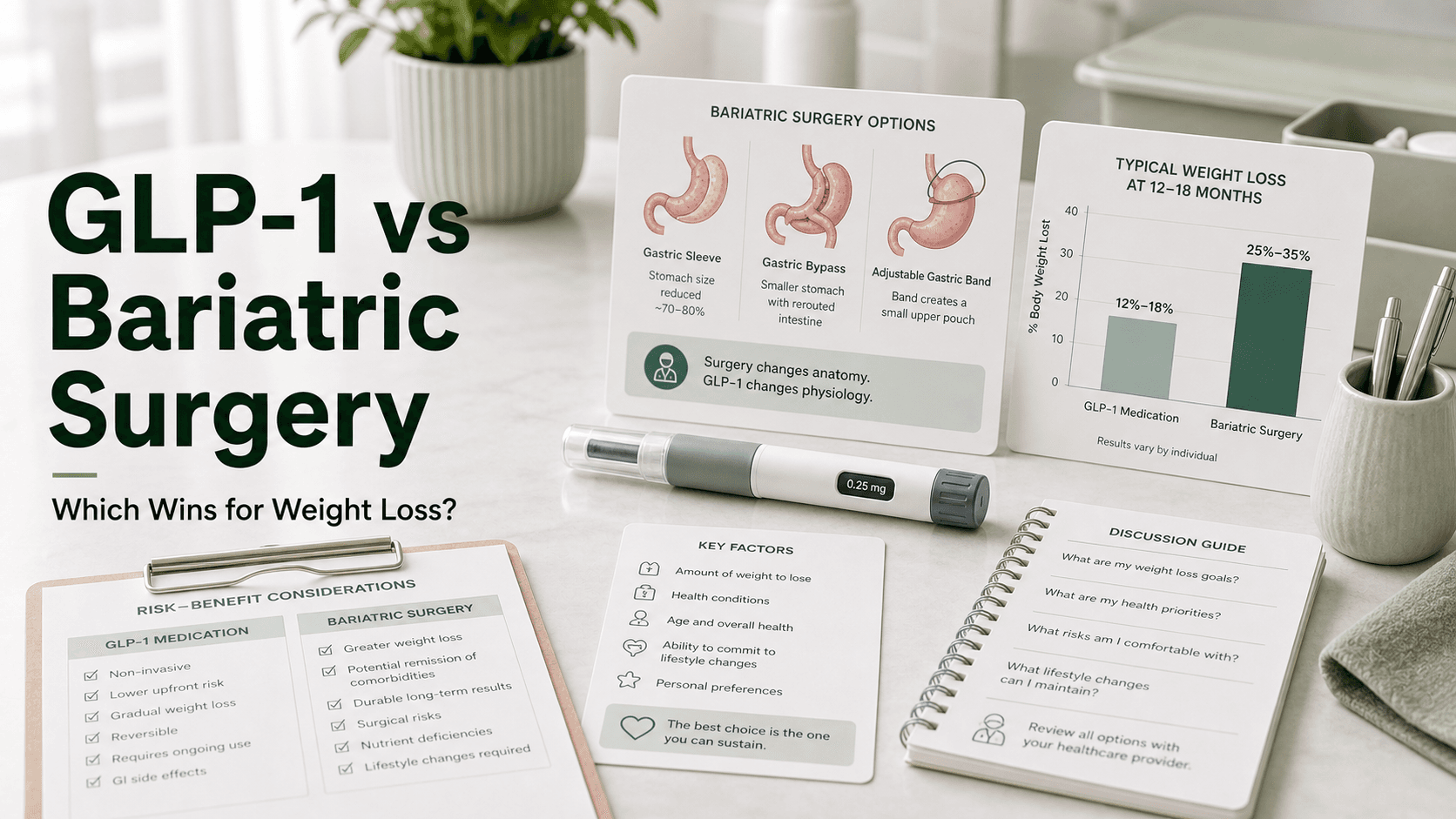
Direct answer: Bariatric surgery produces roughly 25–35% total body weight loss sustained for 5–10+ years. The strongest GLP-1s produce 15–21% weight loss that disappears within a year of stopping. In real-world data, sleeve gastrectomy and gastric bypass beat GLP-1 injections by about 5x at two years (24% vs 4.7% total weight loss). Surgery wins on magnitude and durability. GLP-1s win on accessibility, reversibility, and avoiding an operating room. Many patients now use both — GLP-1 before surgery, or after surgery to push past a plateau.
At a Glance: Surgery vs GLP-1
| Treatment | Mean weight loss | Durability | Up-front cost | Recovery | Reversible | Main risks |
|---|---|---|---|---|---|---|
| Sleeve gastrectomy | ~25% TBWL | 5–10+ years | $15,000–$25,000 | 2–4 weeks | No (anatomically) | Leak, reflux, stricture |
| Gastric bypass (RYGB) | ~30–33% TBWL | 5–10+ years | $20,000–$30,000 | 3–6 weeks | Difficult | Leak, ulcer, dumping, vitamin deficiency |
| Duodenal switch / SADI | ~35–40% TBWL | 5–10+ years | $25,000–$35,000 | 4–6 weeks | No | Malabsorption, diarrhea, nutrient deficiency |
| Adjustable band (Lap-Band) | ~15% TBWL | Often fades by year 5 | $10,000–$18,000 | 1–2 weeks | Yes (removable) | Slippage, erosion, port issues |
| Wegovy (semaglutide) | ~15% TBWL | Only while taking it | $4,000–$15,000/year | None | Yes | Nausea, vomiting, gallstones |
| Zepbound (tirzepatide) | ~20–21% TBWL | Only while taking it | $4,000–$15,000/year | None | Yes | Nausea, vomiting, gallstones |
| Retatrutide (trial) | ~24% TBWL (Phase 2) | Likely while taking it | Not yet priced | None | Yes | Still being characterized |
TBWL = total body weight loss. Cost ranges are U.S. self-pay or post-insurance averages, not guaranteed prices.
The Bariatric Surgery Options
Four procedures account for the vast majority of weight-loss surgery worldwide. Each does something mechanically different to the GI tract.
Sleeve Gastrectomy
The most common bariatric procedure today. About 80% of the stomach is removed, leaving a banana-shaped sleeve. It restricts volume and also drops ghrelin (the hunger hormone) sharply.
- Average loss: ~25% total body weight at 1–2 years
- 5-year sustained loss: ~20–22% TBWL
- 30-day complication rate: ~6.1%
- 30-day mortality: ~0.08%
- Recovery: 2–4 weeks
Roux-en-Y Gastric Bypass
A small pouch is created from the upper stomach and connected directly to the mid-small intestine, bypassing the rest of the stomach and duodenum. Restriction + malabsorption + powerful hormonal changes.
- Average loss: ~30–33% total body weight at 1–2 years
- 5-year sustained loss: ~25–28% TBWL
- Most effective for type 2 diabetes remission of any common procedure
- 30-day complication rate: ~7.9%
- 30-day mortality: ~0.1–0.2%
- Recovery: 3–6 weeks
Duodenal Switch (BPD-DS) and SADI
The most aggressive options. The stomach is sleeved, and a much longer segment of intestine is bypassed. Reserved for patients with the highest BMIs.
- Average loss: ~35–40% total body weight at 1–2 years
- Highest sustained weight loss of any bariatric option
- Highest rates of vitamin and protein deficiency
- Requires lifelong supplementation and monitoring
Adjustable Gastric Band
A silicone band placed around the upper stomach, tightened with saline through a port. Once the dominant procedure; now rarely chosen.
- Average loss: ~15% total body weight
- Weight loss often fades by year 5
- Many bands are eventually removed or converted to sleeve/bypass
- Lowest perioperative risk of the four
- The most reversible procedure
The GLP-1 Options
GLP-1 receptor agonists work systemically — they slow gastric emptying, blunt appetite-related brain signaling, and improve glucose regulation. Three matter for this comparison.
Wegovy (Semaglutide 2.4 mg)
- STEP-1 mean weight loss: 14.9% at 68 weeks
- The only GLP-1 with proven cardiovascular event reduction (SELECT trial)
- Approved for chronic kidney disease in type 2 diabetes
- Weekly subcutaneous injection
Zepbound (Tirzepatide 15 mg)
- SURMOUNT-1 mean weight loss: 20.9% at 72 weeks
- SURMOUNT-5 head-to-head: tirzepatide 20.2% vs semaglutide 13.7%
- Dual GLP-1 + GIP mechanism
- Weekly subcutaneous injection
- Currently the leading FDA-approved drug for absolute weight loss
Retatrutide (Investigational)
- Triple agonist: GLP-1 + GIP + glucagon
- Phase 2 mean weight loss: ~24% at 48 weeks
- Not yet FDA approved; Phase 3 readouts arriving in 2026
- The first medication to approach surgery-level numbers in trials
Weight Loss Head to Head
Trial data and real-world data give somewhat different pictures. Both are worth understanding.
In randomized trial conditions:
- Bariatric surgery (network meta-analysis 2026): roughly 19–28% total weight loss depending on procedure
- Tirzepatide 15 mg: ~21%
- Semaglutide 2.4 mg: ~15%
When trial adherence is perfect, tirzepatide 15 mg is statistically similar to sleeve gastrectomy in some analyses. Roux-en-Y bypass still beats every approved drug.
In real-world conditions:
A 30,000+ patient retrospective study found bariatric surgery patients lost about 5x as much weight as GLP-1 patients at two years: 24% vs 4.7% total weight loss. Why the gap?
- ~70% of GLP-1 patients discontinue within the first year (cost, side effects, access)
- Most never reach the top dose
- Surgery enforces an anatomic change that doesn't require daily compliance
The honest summary: with perfect adherence, modern GLP-1s narrow the gap to surgery. With real-world adherence, surgery wins by a wide margin.
Durability After Stopping
This is the single biggest difference between the two paths.
Bariatric surgery durability:
- Most patients keep the majority of weight off for 5–10+ years
- Some weight regain is normal — typically 5–15% from nadir over a decade
- Anatomic changes (smaller stomach, shorter bowel) don't reverse
GLP-1 durability after stopping:
- The STEP-4 trial measured this directly. Patients who stopped semaglutide regained roughly two-thirds of lost weight within a year.
- Tirzepatide showed similar regain in SURMOUNT-4.
- Hunger hormones, gastric emptying, and food noise return within weeks.
In other words, GLP-1s require indefinite — likely lifelong — use to maintain results. Surgery does not.
A 10-year Cleveland Clinic comparison reported 21.6% sustained weight loss with surgery vs 6.8% with GLP-1 medication, plus a 32% lower mortality risk and 35% lower major adverse cardiac event rate with surgery. Most patients in that cohort stopped their GLP-1 over the decade.
Cost Comparison
Up-front vs ongoing is the key distinction.
Bariatric surgery:
- Self-pay U.S. range: $15,000 (sleeve) to $35,000 (duodenal switch)
- Usually covered by U.S. commercial insurance and Medicare when criteria are met
- One-time cost; minor ongoing costs for vitamins, follow-up, and possible revisions
GLP-1 medications:
- Branded Wegovy or Zepbound list price: ~$1,000/month
- With insurance and savings cards: often $25–$199/month
- Compounded options: $200–$500/month, regulation-dependent
- Yearly cost: $4,000–$15,000 depending on coverage
- Over 10 years of continuous use: $40,000–$150,000
A 2026 cohort study (30,458 patients) found surgery saved about $11,689 in healthcare costs over 2 years vs ongoing GLP-1 therapy, with a break-even point at approximately 15 months from the start of treatment.
If you plan to stay on a GLP-1 for life, the cumulative cost will almost always exceed surgery. If you plan to use a GLP-1 for 1–2 years to lose 30–40 pounds and stop, the math may favor the drug.
Complications and Side Effects
Both options carry meaningful — but very different — risks.
Bariatric surgery risks:
- 30-day mortality: ~0.08% (sleeve) to ~0.2% (bypass) — lower than hip replacement
- 30-day complication rate: 6–8%
- Leaks, bleeding, strictures, ulcers
- Long-term: gallstones, vitamin and mineral deficiencies, dumping syndrome (bypass), reflux (sleeve), small bowel obstruction
- Bone density loss; possible alcohol-use risks after bypass
GLP-1 side effects:
- Nausea, vomiting, diarrhea, constipation — affecting up to 50% at some point
- ~5–10% discontinue for side effects in trials
- Gallbladder disease, pancreatitis, gastroparesis
- Muscle and bone loss without protein and resistance training
- Rare retinal signal (NAION) under investigation with semaglutide
Surgery concentrates risk in a 30-day window with a small but real chance of a serious complication. GLP-1s spread risk thinly across years of daily exposure.
Who Does Each Path Suit Best?
There are no universal rules, but the patterns are clear.
Bariatric surgery is usually the better choice if you:
- Have a BMI of 40+, or 35+ with serious obesity-related disease
- Have type 2 diabetes you want the highest chance of remitting
- Cannot afford or tolerate indefinite medication
- Have tried GLP-1s and stalled below your goal
- Want a durable, one-and-done intervention
- Have a clear support system for post-op recovery
GLP-1s are usually the better choice if you:
- Have a BMI of 27–34.9 with weight-related conditions, or 30–39.9 without surgical desire
- Have surgical contraindications (severe heart or lung disease, certain prior abdominal surgeries)
- Want to avoid an operating room and anatomic change
- Need 10–20% weight loss, not 30–40%
- Have strong insurance coverage or access to affordable compounded options
- Are early in your weight-loss journey and want to try medication first
Both is increasingly common if you:
- Use a GLP-1 before surgery to reduce operative risk and shrink the liver
- Use a GLP-1 after surgery for added loss or to manage regain (more on this below)
- Are awaiting insurance approval for surgery and want to start losing now
Can You Use Both?
Yes — and most major obesity societies now support it.
GLP-1 before surgery. Pre-op weight loss of even 5–10% shrinks the liver, makes surgery technically easier, and improves outcomes. Most centers now allow or require a GLP-1 trial before surgery for higher-BMI patients. The medication is stopped roughly 2 weeks before surgery to reduce aspiration risk from delayed gastric emptying.
GLP-1 after surgery. Up to 25% of bariatric patients have suboptimal weight loss or regain. ASMBS data presented in 2024–2025 show that adding tirzepatide or semaglutide after sleeve or bypass produces an additional 8–15% weight loss in patients who stalled. This is one of the fastest-growing uses of GLP-1s in obesity medicine.
ASMBS President Ann M. Rogers, MD, has stated that patients with insufficient GLP-1 response "should consider bariatric surgery as an option or even in combination."
Switching Between Treatments
From GLP-1 to surgery: Stop the medication ~2 weeks before the operation. Continue a high-protein, low-carbohydrate liver-shrinking diet in the interim.
From surgery to GLP-1: Most centers wait until weight loss plateaus — usually 12–24 months post-op — before considering medication. Earlier use can worsen post-op nausea and complicate nutrient absorption.
Cycling on and off GLP-1: Practical for some people, but expect regain off the drug and re-titration on the way back up.
What People Get Wrong
- "GLP-1s replaced surgery." In real-world data they have not. Surgery still wins on absolute weight loss, durability, mortality, and total cost over time.
- "Bariatric surgery is dangerous." Modern laparoscopic sleeve and bypass have lower mortality than common hip and knee replacements.
- "You can stop the GLP-1 once you hit goal." STEP-4 and SURMOUNT-4 show that most people regain about two-thirds of lost weight within a year of stopping.
- "Surgery is irreversible — the band can be removed." True for the band, but sleeve, bypass, and duodenal switch are anatomically permanent for practical purposes.
- "Tirzepatide equals surgery." In carefully controlled trials, tirzepatide narrows the gap. In the real world, surgery still outperforms because so many patients can't sustain medication long-term.
- "Combining doesn't work." It does — ASMBS data support GLP-1 use before and after surgery for selected patients.
Frequently Asked Questions
Does GLP-1 work as well as gastric sleeve? Not on average. Sleeve produces ~25% total body weight loss; Wegovy ~15% and Zepbound ~20–21%. Tirzepatide narrows the gap most in trials, but real-world adherence usually widens it.
Is tirzepatide as good as gastric bypass? Tirzepatide reaches ~21% in trials; gastric bypass averages ~30–33%. Bypass also produces stronger diabetes remission.
Will I regain weight if I stop my GLP-1? Most likely yes. Trial data show about two-thirds of lost weight is regained within a year of stopping semaglutide or tirzepatide.
Is bariatric surgery cheaper than Wegovy long term? Usually yes. Break-even is around 15 months. Over a decade, GLP-1 therapy commonly costs $40,000–$150,000; surgery is a one-time $15,000–$30,000.
Can I take Wegovy or Zepbound after gastric sleeve? Yes, typically after 12–24 months post-op if weight has plateaued or regain has started. Many bariatric programs now offer this.
Do I have to stop GLP-1 before surgery? Yes. Most centers stop the drug ~2 weeks before any procedure under anesthesia because of delayed gastric emptying and aspiration risk.
Which is safer: GLP-1 or bariatric surgery? Surgery has a small concentrated risk in a 30-day window (~0.1% mortality, 6–8% complications). GLP-1s have a low but ongoing daily side effect burden. Long-term mortality in observational data favors surgery in patients with severe obesity.
Last reviewed: May 13, 2026
Sources
- Obesity Treatment With Bariatric Surgery vs GLP-1 Receptor Agonists — JAMA Surgery
- Head-to-head Study Shows Bariatric Surgery Superior to GLP-1 Drugs for Weight Loss — ASMBS
- Bariatric Surgery vs. GLP-1 Medications: What the Latest Research Shows — ASMBS
- 2025 Metabolic and Bariatric Surgery Fact Sheet — ASMBS
- GLP-1 drugs versus bariatric surgery for treating obesity — Harvard Health
- New Study Finds Bariatric Surgery Associated with Greater Benefits Than GLP-1RAs Alone — Cleveland Clinic
- Comparative Efficacy of Metabolic/Bariatric Surgery Versus GLP-1 Receptor Agonists: Network Meta-Analysis — Obesity (Wiley)
- Navigating weight loss: When to consider bariatric surgery after GLP-1 therapy — UChicago Medicine
- Weight Loss Medication or Weight Loss Surgery? — UCLA Health
- 30-day morbidity and mortality of sleeve gastrectomy, RYGB and OAGB — International Journal of Obesity (Nature)




