


Gastroparesis is the GLP-1 complication that drives the most headlines, the most lawsuits, and the most fear. It is also the side effect most often confused with the routine, expected slowing of stomach emptying that every GLP-1 patient experiences. The honest answer requires separating two very different things: the universal, transient delay in gastric emptying that defines how these drugs work, and the rare but serious clinical syndrome of chronic gastroparesis that can persist for months.
Delayed gastric emptying is exactly why doctors give guidance on GLP-1 use before procedures.
Direct answer: GLP-1 receptor agonists raise the relative risk of a formal gastroparesis diagnosis roughly 3 to 4 times versus comparator therapies in published cohorts — about 6.5 cases per 1,000 person-years on semaglutide versus 2.1 on bupropion–naltrexone in obesity patients, with a hazard ratio of 3.33 (95% CI 2.27–4.98) vs. bupropion–naltrexone and 6.14 (3.94–9.57) vs. sleeve gastrectomy. A separate University of British Columbia analysis found a 3.67× higher risk with an incidence of 0.53%. Absolute risk remains under 1%, and most cases resolve within 4 to 8 weeks of stopping the drug as it clears. A small but real subset develops persistent symptoms. As of May 2026, MDL-3094 in the Eastern District of Pennsylvania (Judge Karen S. Marston) contains roughly 3,546–3,636 active cases, with bellwether selection in expert discovery. Anesthesia guidelines now require holding weekly GLP-1s for 7 days and daily formulations for 24 hours before procedures with sedation.
Gastroparesis vs. Delayed Gastric Emptying: The Distinction That Matters
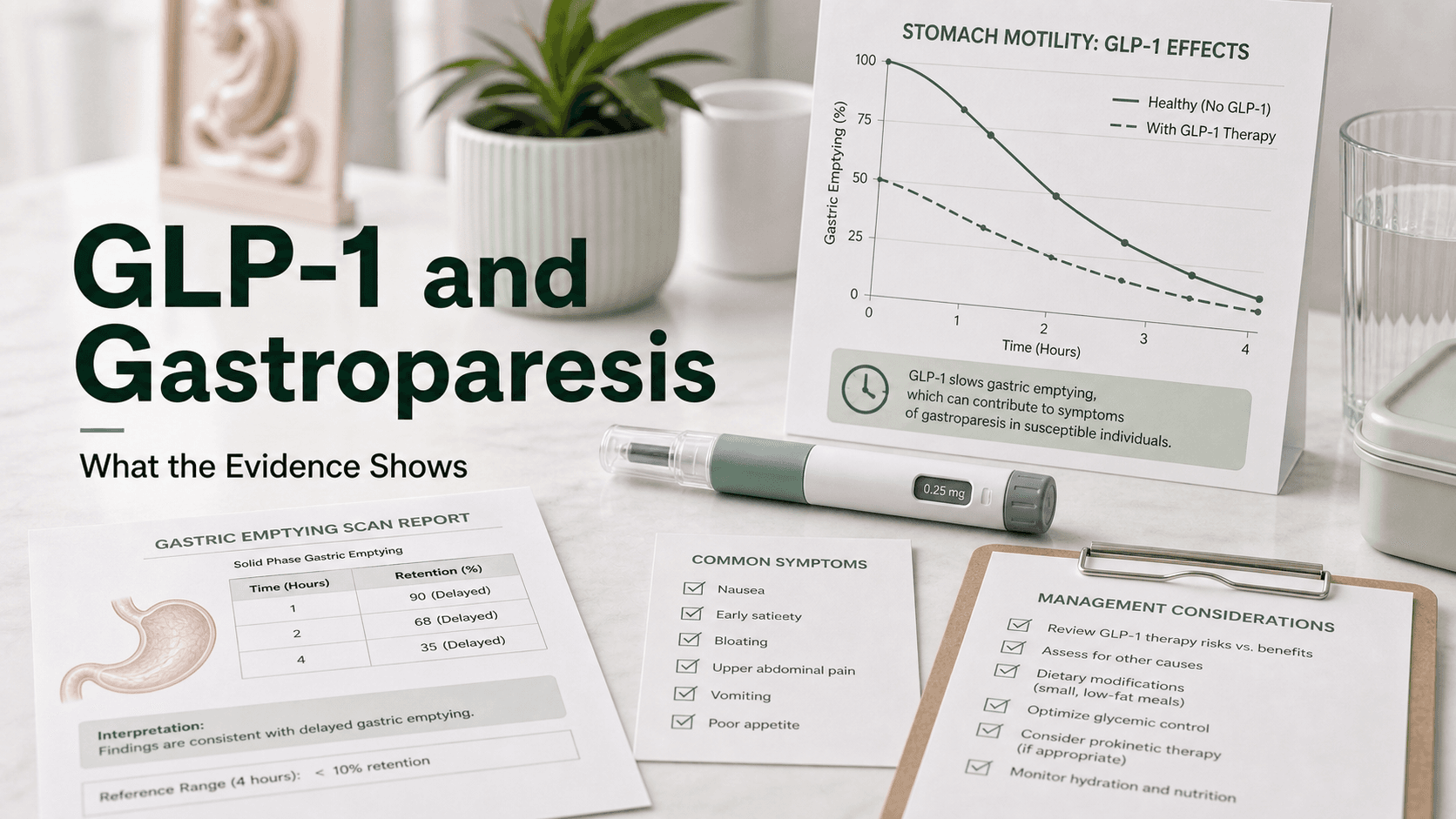
Every GLP-1 user has delayed gastric emptying. That is not a side effect — it is the mechanism. Slower stomach emptying is how these drugs flatten post-meal glucose spikes and prolong satiety. The clinically relevant question is whether that delay becomes pathologic.
- Transient delayed gastric emptying is universal on GLP-1s. It is most pronounced after the first few doses and diminishes substantially over 4 to 16 weeks through a tachyphylaxis effect (the receptor adapts to sustained activation). Most patients feel some fullness, mild nausea, or reduced appetite. This is expected and resolves with dose stability.
- Chronic gastroparesis is a distinct clinical syndrome: persistent delayed emptying confirmed on objective testing, with symptoms severe enough to impair nutrition, hydration, or quality of life. By formal criteria, this is uncommon — roughly 0.5–0.7% of users in the published cohorts — but it is the form that triggers hospital visits, weight failure, and litigation.
A 2024 endoscopy series found retained gastric contents in 13.6% of GLP-1 users versus 2.3% of non-users (a roughly 4-fold increase), confirming that meaningful gastric retention is common even when patients are not symptomatic enough to seek care.
Symptoms of GLP-1 Gastroparesis
Symptoms exist on a spectrum from "mild and expected" to "ER-worthy." Concerning features include:
- Vomiting for four or more weeks — the threshold most plaintiff attorneys use for MDL eligibility
- Postprandial fullness that persists hours after eating small portions
- Early satiety progressing to inability to finish even a few bites
- Severe bloating with visible upper-abdominal distension
- Recurrent vomiting of undigested food eaten hours earlier
- Cyclical nausea that does not improve with antiemetics or dose holds
- Unintended weight loss beyond the expected trajectory with dehydration or electrolyte derangements
- Sulfur ("rotten egg") burps from prolonged fermentation in a stagnant stomach
Routine GLP-1 nausea typically improves within 2 to 4 weeks of dose stability. Symptoms that worsen, persist beyond 8 weeks, or cause weight failure deserve evaluation.
How Gastroparesis Is Diagnosed
Imaging and endoscopy can rule out obstruction but cannot diagnose gastroparesis. Three motility tests can.
Gastric Emptying Scintigraphy (the Gold Standard)
A nuclear medicine study using a technetium-99m-labeled low-fat solid meal (egg whites, jam, toast, and water). Scans at 0, 60, 120, 180, and 240 minutes track radioactive retention.
Diagnostic thresholds per the American College of Gastroenterology:
- Greater than 60% retention at 2 hours, or
- Greater than 10% retention at 4 hours
Studies shorter than three hours produce false negatives and are not recommended. The four-hour protocol is 30% more sensitive than two-hour studies.
Wireless Motility Capsule (SmartPill)
A swallowed capsule transmits pH, pressure, and temperature data as it traverses the GI tract. It measures gastric emptying time and full transit time. Useful when scintigraphy is unavailable or when small-bowel and colonic motility data are also needed.
13C-Spirulina Breath Test
A meal labeled with stable (non-radioactive) carbon-13 spirulina. As the meal empties and is metabolized, 13CO2 appears in exhaled breath. Correlates well with scintigraphy and avoids radiation — useful for pregnant patients or pediatrics.
CT, MRI, ultrasound, and upper endoscopy cannot diagnose gastroparesis. They are used to exclude mechanical obstruction, gastric outlet narrowing, ulcers, or malignancy before a motility study.
Who Is at Higher Risk
Not every GLP-1 user has the same risk profile. Factors associated with higher gastroparesis incidence:
- Pre-existing type 2 diabetes, especially long-standing or poorly controlled (autonomic neuropathy of the vagus nerve is the leading non-drug cause of gastroparesis)
- Rapid dose escalation — published case reports specifically tie symptomatic gastroparesis to skipping the standard titration intervals
- Higher doses of semaglutide (1.7 mg, 2.4 mg) and tirzepatide (10–15 mg)
- Concurrent opioids, anticholinergics, or tricyclics that independently slow motility
- Prior gastric surgery or vagus nerve injury
- Female sex (background gastroparesis is roughly 4× more common in women)
- History of cyclic vomiting syndrome, migraine, or functional dyspepsia
A pre-existing motility disorder is a strong relative contraindication. Patients with known idiopathic or diabetic gastroparesis should not start a GLP-1 without specialist input.
Reversibility: What Happens After You Stop
This is the most clinically important question, and the answer is reassuring for the majority.
- Semaglutide's half-life is about 7 days. Substantial drug elimination takes 4 to 5 weeks.
- Tirzepatide's half-life is about 5 days. Similar elimination window.
- Symptom resolution typically occurs within 4 to 8 weeks of discontinuation in patients without a pre-existing motility disorder.
- A small subset experiences persistent symptoms for months. Most published case series describe eventual recovery, but timelines of 6 to 12 months are reported.
Mechanism matters: GLP-1-induced gastroparesis is from ongoing receptor activation, not nerve damage. Once the drug is gone, receptor signaling stops. This is fundamentally different from the irreversible vagal denervation that causes diabetic or post-surgical gastroparesis. That mechanistic difference is why most patients recover.
Pre-existing diabetic neuropathy can confound recovery — when GLP-1 unmasks underlying diabetic gastroparesis, symptoms may not fully resolve because the baseline pathology is still present.
MDL-3094: The Legal Background
The federal multidistrict litigation is the second-largest GLP-1 case grouping in the country and the primary venue for gastroparesis claims.
- Court: U.S. District Court, Eastern District of Pennsylvania
- Judge: Karen S. Marston
- Case count (May 2026): approximately 3,546–3,636 active personal injury suits
- Stage: Expert discovery; bellwether trial selection expected late 2026
- Claim distribution: ~75% gastroparesis or stomach paralysis, ~18% ileus, ~8% gallbladder, with some overlap
- Core allegation: Failure to warn — that Novo Nordisk and Eli Lilly knew or should have known about elevated gastroparesis risk and provided inadequate label warnings
The MDL does not resolve causation. It examines whether label warnings were adequate at the time of prescription. A separate MDL, MDL-3163, was created in December 2025 for NAION vision-loss cases and is also venued before Judge Marston in EDPA.
Anesthesia and Surgery Implications
Retained gastric contents during induction of general anesthesia can lead to regurgitation and pulmonary aspiration — a rare but potentially fatal complication. Three guidelines now address this:
- American Society of Anesthesiologists (ASA) 2023 consensus: Hold weekly GLP-1s for 7 days and daily formulations for 24 hours before elective procedures with sedation or general anesthesia.
- Multi-society 2024 update (ASA, AGA, AASLD, ASGE, ISPAD): Risk-stratified. Low-risk elective procedures may continue therapy; high-risk patients (recent dose escalation, ongoing GI symptoms, large meals before NPO window) should follow a 24-hour clear-liquid diet and consider holding.
- SPAQI consensus statement: Point-of-care gastric ultrasound can assess residual gastric contents when in doubt.
Patients on GLP-1s who present to an ER for emergent surgery should explicitly tell the anesthesiologist. Rapid-sequence induction, smaller meals before the NPO window, or regional anesthesia may be safer choices.
Diagnostic Criteria for MDL-3094 Eligibility
Plaintiff law firms have moved from accepting symptom-based screens to requiring objective diagnostic evidence. As of 2026, viable claims generally require:
- A confirmed gastroparesis diagnosis by ICD-10 code (K31.84) supported by:
- Gastric emptying scintigraphy showing >60% retention at 2 hours or >10% at 4 hours, or
- Wireless motility capsule confirming delayed emptying, or
- 13C-spirulina breath test consistent with gastroparesis
- Symptoms of at least four weeks of recurrent vomiting (the working threshold most firms use)
- Documented GLP-1 use in the 30 days preceding the diagnostic study
- Exclusion of alternative causes — obstruction, prior gastric surgery, pre-existing diabetic gastroparesis (in some cases), opioid use sufficient to explain symptoms
- Records demonstrating prescribing physician notification of symptoms
Endoscopy, CT, and MRI alone do not satisfy these criteria, even if they document retained food. Motility data is what now distinguishes accepted from rejected screens.
Management Strategies
For symptomatic patients, the management ladder is roughly:
- Reduce or hold the dose. The first step. Most early-stage gastroparesis responds to dose reduction or temporary discontinuation.
- Small, frequent meals. Five to six small meals; avoid large evening meals.
- Low-fat, low-fiber, low-residue diet. Fat and fiber both slow emptying further.
- Liquids and purees preferentially. Liquid emptying is preserved even when solid emptying fails.
- Adequate hydration with electrolytes. Vomiting cycles cause rapid sodium, potassium, and chloride losses.
- Prokinetics if symptoms warrant. Metoclopramide (with the black-box warning for tardive dyskinesia in mind) or domperidone where available. Erythromycin can help acutely.
- Antiemetics for symptom control. Ondansetron is first-line.
- Specialist referral. Persistent or severe cases warrant gastroenterology evaluation and a motility study before any dose changes that might mask findings.
- Discontinuation if persistent. For severe, prolonged symptoms with weight failure or dehydration, stopping the drug is the right answer even if it means losing the weight benefit.
Most patients do not need all of these steps. Dose reduction and dietary changes resolve most symptoms within weeks.
What People Get Wrong About GLP-1 Gastroparesis
- "Any nausea on Ozempic means I have gastroparesis." Mild to moderate nausea in the first 4 weeks of each dose step is expected. It is not gastroparesis.
- "Gastroparesis from Ozempic is permanent." The majority of cases resolve within 4 to 8 weeks of stopping. Persistent cases exist but are the minority.
- "My CT scan ruled out gastroparesis." CT cannot diagnose or exclude gastroparesis. Only motility testing can.
- "Tirzepatide is safer than semaglutide for the stomach." Direct head-to-head data is limited. Both delay gastric emptying. Some analyses show similar gastroparesis signals; others suggest tirzepatide may be modestly better tolerated.
- "I should stop my GLP-1 before any procedure." For low-risk elective procedures in patients without GI symptoms, current multi-society guidance allows continuation. The decision should involve your anesthesiologist.
- "The lawsuit means GLP-1s are unsafe." MDL-3094 is examining the adequacy of warning labels, not whether the drugs should be withdrawn. Tens of millions of patients use them safely.
Frequently Asked Questions
Can Ozempic cause stomach paralysis? GLP-1 medications including semaglutide are associated with a roughly 3 to 4-fold relative increase in gastroparesis diagnosis. Absolute risk is under 1% in published cohorts. The condition usually resolves after stopping the drug.
What is the difference between Ozempic stomach paralysis and normal Ozempic nausea? Normal nausea is mild, dose-related, and improves within 2 to 4 weeks. Gastroparesis features persistent vomiting, severe bloating, vomiting of undigested food, and inability to tolerate normal portions for more than 4 weeks.
How is GLP-1 gastroparesis diagnosed? A gastric emptying scintigraphy (the gold standard), wireless motility capsule, or 13C-spirulina breath test. Gastric retention greater than 60% at 2 hours or greater than 10% at 4 hours confirms delayed emptying.
Is GLP-1 gastroparesis reversible? For most patients, yes. Symptoms typically improve within 4 to 8 weeks of stopping, in parallel with drug elimination. A small minority experiences persistent symptoms, particularly those with pre-existing diabetic neuropathy.
Do I have to stop my GLP-1 before surgery? Per current ASA guidance, hold weekly formulations for 7 days and daily formulations for 24 hours before procedures with sedation or general anesthesia. Multi-society 2024 guidance individualizes the decision based on aspiration risk.
Do I qualify for the Ozempic gastroparesis lawsuit? Most firms in MDL-3094 require a formal gastroparesis diagnosis confirmed by motility testing, at least 4 weeks of vomiting, documented GLP-1 use in the prior 30 days, and exclusion of obvious alternative causes. Symptom screens alone are no longer sufficient.
Last reviewed: May 13, 2026
Sources
- Comparing the risk of gastroparesis following different GLP-1 receptor agonists — PMC
- Increased Risk of Gastroparesis Associated with GLP-1RA Use in Patients with T2DM — Cleveland Clinic Consult QD
- Clinical Consequences of Delayed Gastric Emptying With GLP-1 RAs and Tirzepatide — JCEM
- What Patients Should Know About GLP-1s and Gastroparesis — National Jewish Health
- Ozempic Lawsuit — Drugwatch May 2026 Update
- The 2026 Ozempic Litigation Pivot: From Symptoms to Scintigraphy — Mohr Marketing
- ASA Consensus-Based Guidance on Preoperative Management of Patients on GLP-1 Receptor Agonists
- Multisociety Clinical Practice Guidance for the Safe Use of GLP-1 RAs in the Perioperative Period — CGH
- Gastric Emptying Scan — StatPearls / NCBI
- Gold Standard Diagnostic Test Underutilized for Gastroparesis — Cleveland Clinic Consult QD




